

Glucocorticoid
Encyclopedia
Steroid hormone
A steroid hormone is a steroid that acts as a hormone. Steroid hormones can be grouped into five groups by the receptors to which they bind: glucocorticoids, mineralocorticoids, androgens, estrogens, and progestogens...
s that bind to the glucocorticoid receptor
Glucocorticoid receptor
The glucocorticoid receptor also known as NR3C1 is the receptor to which cortisol and other glucocorticoids bind....
(GR), which is present in almost every vertebrate
Vertebrate
Vertebrates are animals that are members of the subphylum Vertebrata . Vertebrates are the largest group of chordates, with currently about 58,000 species described. Vertebrates include the jawless fishes, bony fishes, sharks and rays, amphibians, reptiles, mammals, and birds...
animal cell. The name glucocorticoid (glucose + cortex + steroid) derives from their role in the regulation of the metabolism of glucose
Glucose
Glucose is a simple sugar and an important carbohydrate in biology. Cells use it as the primary source of energy and a metabolic intermediate...
, their synthesis in the adrenal cortex
Adrenal cortex
Situated along the perimeter of the adrenal gland, the adrenal cortex mediates the stress response through the production of mineralocorticoids and glucocorticoids, including aldosterone and cortisol respectively. It is also a secondary site of androgen synthesis.-Layers:Notably, the reticularis in...
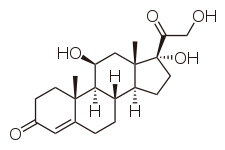
, and their steroid
Steroid
A steroid is a type of organic compound that contains a characteristic arrangement of four cycloalkane rings that are joined to each other. Examples of steroids include the dietary fat cholesterol, the sex hormones estradiol and testosterone, and the anti-inflammatory drug dexamethasone.The core...
al structure (see structure to the right).
GCs are part of the feedback mechanism in the immune system
Immune system
An immune system is a system of biological structures and processes within an organism that protects against disease by identifying and killing pathogens and tumor cells. It detects a wide variety of agents, from viruses to parasitic worms, and needs to distinguish them from the organism's own...
that turns immune activity (inflammation
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
) down. They are therefore used in medicine to treat diseases that are caused by an overactive immune system, such as allergies, asthma, autoimmune diseases and sepsis. GCs have many diverse (pleiotropic
Pleiotropy (drugs)
In pharmacology, pleiotropy refers to a drug's actions, usually unanticipated, other than those for which the agent was specifically developed. It may include adverse effects which are detrimental ones, but is often used to denote additional beneficial effects....
) effects, including potentially harmful side effects, and as a result are rarely sold over-the-counter. They also interfere with some of the abnormal mechanisms in cancer
Cancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
cells, so they are used in high doses to treat cancer.
GCs cause their effects by binding to the glucocorticoid receptor
Glucocorticoid receptor
The glucocorticoid receptor also known as NR3C1 is the receptor to which cortisol and other glucocorticoids bind....
(GR). The activated GR complex in turn up-regulates the expression of anti-inflammatory proteins in the nucleus
Cell nucleus
In cell biology, the nucleus is a membrane-enclosed organelle found in eukaryotic cells. It contains most of the cell's genetic material, organized as multiple long linear DNA molecules in complex with a large variety of proteins, such as histones, to form chromosomes. The genes within these...
(a process known as transactivation
Transactivation
In molecular biology and genetics, transactivation is an increased rate of gene expression triggered either by biological processes or by artificial means.- Natural transactivation :...
) and represses the expression of pro-inflammatory proteins in the cytosol
Cytosol
The cytosol or intracellular fluid is the liquid found inside cells, that is separated into compartments by membranes. For example, the mitochondrial matrix separates the mitochondrion into compartments....
by preventing the translocation
Protein targeting
Protein targeting or protein sorting is the mechanism by which a cell transports proteins to the appropriate positions in the cell or outside of it. Sorting targets can be the inner space of an organelle, any of several interior membranes, the cell's outer membrane, or its exterior via secretion...
of other transcription factor
Transcription factor
In molecular biology and genetics, a transcription factor is a protein that binds to specific DNA sequences, thereby controlling the flow of genetic information from DNA to mRNA...
s from the cytosol into the nucleus (transrepression
Transrepression
In the field of molecular biology, transrepression is a process whereby one protein represses the activity of a second protein through a protein-protein interaction...
).
Glucocorticoids are distinguished from mineralocorticoid
Mineralocorticoid
Mineralocorticoids are a class of steroid hormones characterised by their similarity to aldosterone and their influence on salt and water balances.-Physiology:...
s and sex steroid
Sex steroid
Sex steroids, also known as gonadal steroids, are steroid hormones that interact with vertebrate androgen or estrogen receptors. Their effects are mediated by slow genomic mechanisms through nuclear receptors as well as by fast nongenomic mechanisms through membrane-associated receptors and...
s by their specific receptors, target cells, and effects. In technical terms, corticosteroid
Corticosteroid
Corticosteroids are a class of steroid hormones that are produced in the adrenal cortex. Corticosteroids are involved in a wide range of physiologic systems such as stress response, immune response and regulation of inflammation, carbohydrate metabolism, protein catabolism, blood electrolyte...
refers to both glucocorticoids and mineralocorticoids (as both are mimics of hormones produced by the adrenal cortex
Adrenal cortex
Situated along the perimeter of the adrenal gland, the adrenal cortex mediates the stress response through the production of mineralocorticoids and glucocorticoids, including aldosterone and cortisol respectively. It is also a secondary site of androgen synthesis.-Layers:Notably, the reticularis in...
), but is often used as a synonym for glucocorticoid.
Cortisol
Cortisol
Cortisol is a steroid hormone, more specifically a glucocorticoid, produced by the adrenal gland. It is released in response to stress and a low level of blood glucocorticoids. Its primary functions are to increase blood sugar through gluconeogenesis; suppress the immune system; and aid in fat,...
(or hydrocortisone) is the most important human glucocorticoid. It is essential for life, and it regulates or supports a variety of important cardiovascular, metabolic
Metabolism
Metabolism is the set of chemical reactions that happen in the cells of living organisms to sustain life. These processes allow organisms to grow and reproduce, maintain their structures, and respond to their environments. Metabolism is usually divided into two categories...
, immunologic
Immunology
Immunology is a broad branch of biomedical science that covers the study of all aspects of the immune system in all organisms. It deals with the physiological functioning of the immune system in states of both health and diseases; malfunctions of the immune system in immunological disorders ; the...
, and homeostatic
Homeostasis
Homeostasis is the property of a system that regulates its internal environment and tends to maintain a stable, constant condition of properties like temperature or pH...
functions. Various synthetic glucocorticoids are available; these are used either as replacement therapy in glucocorticoid deficiency or to suppress the immune system.
Effects
Immunology
Immunology is a broad branch of biomedical science that covers the study of all aspects of the immune system in all organisms. It deals with the physiological functioning of the immune system in states of both health and diseases; malfunctions of the immune system in immunological disorders ; the...
and metabolic
Metabolism
Metabolism is the set of chemical reactions that happen in the cells of living organisms to sustain life. These processes allow organisms to grow and reproduce, maintain their structures, and respond to their environments. Metabolism is usually divided into two categories...
. In addition, glucocorticoids play important roles in fetal development
Developmental biology
Developmental biology is the study of the process by which organisms grow and develop. Modern developmental biology studies the genetic control of cell growth, differentiation and "morphogenesis", which is the process that gives rise to tissues, organs and anatomy.- Related fields of study...
.
Immune
As discussed in more detail below, glucocorticoids function through interaction with the glucocorticoid receptor:- up-regulate the expression of anti-inflammatory proteins
- down-regulate the expression of pro-inflammatory proteins
Glucocorticoids are also shown to play a role in the development and homeostasis of T lymphocytes. This has been shown in the transgenic mice with either increased or decreased sensitivity of T cell lineage to glucocorticoids.
Metabolic
The name "glucocorticoid" derives from early observations that these hormoneHormone
A hormone is a chemical released by a cell or a gland in one part of the body that sends out messages that affect cells in other parts of the organism. Only a small amount of hormone is required to alter cell metabolism. In essence, it is a chemical messenger that transports a signal from one...
s were involved in glucose metabolism. In the fasted state, cortisol
Cortisol
Cortisol is a steroid hormone, more specifically a glucocorticoid, produced by the adrenal gland. It is released in response to stress and a low level of blood glucocorticoids. Its primary functions are to increase blood sugar through gluconeogenesis; suppress the immune system; and aid in fat,...
stimulates several processes that collectively serve to increase and maintain normal concentrations of glucose in blood.
Metabolic effects:
- Stimulation of gluconeogenesisGluconeogenesisGluconeogenesis is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and glucogenic amino acids....
, in particular, in the liverLiverThe liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion...
: This pathway results in the synthesis of glucose from non-hexoseHexoseIn organic chemistry, a hexose is a monosaccharide with six carbon atoms, having the chemical formula C6H12O6. Hexoses are classified by functional group, with aldohexoses having an aldehyde at position 1, and ketohexoses having a ketone at position 2....
substrates such as amino acidAmino acidAmino acids are molecules containing an amine group, a carboxylic acid group and a side-chain that varies between different amino acids. The key elements of an amino acid are carbon, hydrogen, oxygen, and nitrogen...
s and glycerolGlycerolGlycerol is a simple polyol compound. It is a colorless, odorless, viscous liquid that is widely used in pharmaceutical formulations. Glycerol has three hydroxyl groups that are responsible for its solubility in water and its hygroscopic nature. The glycerol backbone is central to all lipids...
from triglyceride breakdown, and is particularly important in carnivoreCarnivoreA carnivore meaning 'meat eater' is an organism that derives its energy and nutrient requirements from a diet consisting mainly or exclusively of animal tissue, whether through predation or scavenging...
s and certain herbivoreHerbivoreHerbivores are organisms that are anatomically and physiologically adapted to eat plant-based foods. Herbivory is a form of consumption in which an organism principally eats autotrophs such as plants, algae and photosynthesizing bacteria. More generally, organisms that feed on autotrophs in...
s. Enhancing the expression of enzymeEnzymeEnzymes are proteins that catalyze chemical reactions. In enzymatic reactions, the molecules at the beginning of the process, called substrates, are converted into different molecules, called products. Almost all chemical reactions in a biological cell need enzymes in order to occur at rates...
s involved in gluconeogenesisGluconeogenesisGluconeogenesis is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and glucogenic amino acids....
is probably the best-known metabolic function of glucocorticoids. - Mobilization of amino acidAmino acidAmino acids are molecules containing an amine group, a carboxylic acid group and a side-chain that varies between different amino acids. The key elements of an amino acid are carbon, hydrogen, oxygen, and nitrogen...
s from extrahepatic tissues: These serve as substrates for gluconeogenesisGluconeogenesisGluconeogenesis is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and glucogenic amino acids....
. - Inhibition of glucose uptake in muscle and adipose tissue: A mechanism to conserve glucose.
- Stimulation of fat breakdown in adipose tissue: The fatty acids released by lipolysisLipolysisLipolysis is the breakdown of lipids and involves the hydrolysis of triglycerides into free fatty acids followed by further degradation into acetyl units by beta oxidation. The process produces Ketones, which are found in large quantities in ketosis, a metabolic state that occurs when the liver...
are used for production of energy in tissues like muscle, and the released glycerolGlycerolGlycerol is a simple polyol compound. It is a colorless, odorless, viscous liquid that is widely used in pharmaceutical formulations. Glycerol has three hydroxyl groups that are responsible for its solubility in water and its hygroscopic nature. The glycerol backbone is central to all lipids...
provide another substrate for gluconeogenesis.
Excessive glucocorticoid levels resulting from administration as a drug or hyperadrenocorticism
Cushing's syndrome
Cushing's syndrome is a hormone disorder caused by high levels of cortisol in the blood. This can be caused by taking glucocorticoid drugs, or by tumors that produce cortisol or adrenocorticotropic hormone or CRH...
have effects on many systems. Some examples include inhibition of bone formation, suppression of calcium absorption (both of which can lead to osteoporosis
Osteoporosis
Osteoporosis is a disease of bones that leads to an increased risk of fracture. In osteoporosis the bone mineral density is reduced, bone microarchitecture is deteriorating, and the amount and variety of proteins in bone is altered...
), delayed wound healing, muscle weakness, and increased risk of infection. These observations suggest a multitude of less-dramatic physiologic roles for glucocorticoids.
Developmental
Glucocorticoids have multiple effects on fetal development. An important example is their role in promoting maturation of the lung and production of the surfactantSurfactant
Surfactants are compounds that lower the surface tension of a liquid, the interfacial tension between two liquids, or that between a liquid and a solid...
necessary for extrauterine lung function. Mice with homozygous disruptions in the corticotropin-releasing hormone gene (see below) die at birth due to pulmonary immaturity. In addition, glucocorticoids are necessary for normal brain development, by initiating terminal maturation, remodeling axons and dendrites, and affecting cell survival.
Arousal and cognition
Hippocampus
The hippocampus is a major component of the brains of humans and other vertebrates. It belongs to the limbic system and plays important roles in the consolidation of information from short-term memory to long-term memory and spatial navigation. Humans and other mammals have two hippocampi, one in...
, amygdala
Amygdala
The ' are almond-shaped groups of nuclei located deep within the medial temporal lobes of the brain in complex vertebrates, including humans. Shown in research to perform a primary role in the processing and memory of emotional reactions, the amygdalae are considered part of the limbic system.-...
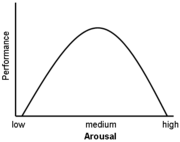
, and frontal lobes. Along with adrenaline, these enhance the formation of flashbulb memories of events associated with strong emotions both positive and negative. This has been confirmed in studies, whereby blockade of either glucocorticoids or noradrenaline activity impaired the recall of emotionally relevant information. Additional sources have shown that subjects whose fear learning was accompanied by high cortisol levels had better consolidation of this memory (this effect was more important in men). Glucocorticoids have also been shown to have a significant impact on vigilance and cognitive performance. This appears to follow the Yerkes-Dodson Curve, as studies have shown that circulating levels of glucocorticoids vs. memory performance follow an upside-down U pattern, much like the Yerkes-Dodson curve. For example, long-term potentiation
Long-term potentiation
In neuroscience, long-term potentiation is a long-lasting enhancement in signal transmission between two neurons that results from stimulating them synchronously. It is one of several phenomena underlying synaptic plasticity, the ability of chemical synapses to change their strength...
(the process of forming long-term memories) is optimal when glucocorticoid levels are mildly elevated, whereas significant decreases of LTP are observed after adrenalectomy (low-GC state) or after exogenous glucocorticoid administration (high-GC state). It has also been shown that elevated levels of glucocorticoids enhance memory for emotionally arousing events, but lead more often than not to poor memory for material unrelated to the source of stress/emotional arousal. In contrast to the dose-dependent enhancing effects of glucocorticoids on memory consolidation, these stress hormones have been shown to inhibit the retrieval of already stored information.
Transactivation
Glucocorticoids bind to the cytosolic glucocorticoid receptorGlucocorticoid receptor
The glucocorticoid receptor also known as NR3C1 is the receptor to which cortisol and other glucocorticoids bind....
(GR). This type of receptor
Receptor (biochemistry)
In biochemistry, a receptor is a molecule found on the surface of a cell, which receives specific chemical signals from neighbouring cells or the wider environment within an organism...
is activated by ligand
Ligand
In coordination chemistry, a ligand is an ion or molecule that binds to a central metal atom to form a coordination complex. The bonding between metal and ligand generally involves formal donation of one or more of the ligand's electron pairs. The nature of metal-ligand bonding can range from...
binding. After a hormone binds to the corresponding receptor, the newly formed receptor-ligand complex translocates itself into the cell nucleus
Cell nucleus
In cell biology, the nucleus is a membrane-enclosed organelle found in eukaryotic cells. It contains most of the cell's genetic material, organized as multiple long linear DNA molecules in complex with a large variety of proteins, such as histones, to form chromosomes. The genes within these...
, where it binds to glucocorticoid response elements (GRE) in the promoter region of the target gene
Gene
A gene is a molecular unit of heredity of a living organism. It is a name given to some stretches of DNA and RNA that code for a type of protein or for an RNA chain that has a function in the organism. Living beings depend on genes, as they specify all proteins and functional RNA chains...
s resulting in the regulation
Downregulation and upregulation
Downregulation is the process by which a cell decreases the quantity of a cellular component, such as RNA or protein, in response to an external variable...
of gene expression
Regulation of gene expression
Gene modulation redirects here. For information on therapeutic regulation of gene expression, see therapeutic gene modulation.Regulation of gene expression includes the processes that cells and viruses use to regulate the way that the information in genes is turned into gene products...
. This process is commonly referred to as transactivation
Transactivation
In molecular biology and genetics, transactivation is an increased rate of gene expression triggered either by biological processes or by artificial means.- Natural transactivation :...
.
The proteins encoded by these upregulated genes have a wide range of effects including for example:
- anti-inflammatoryAnti-inflammatoryAnti-inflammatory refers to the property of a substance or treatment that reduces inflammation. Anti-inflammatory drugs make up about half of analgesics, remedying pain by reducing inflammation as opposed to opioids, which affect the central nervous system....
– lipocortin IAnnexinAnnexin is a common name for a group of cellular proteins. They are found in all kingdoms with the exception of the bacteria....
, p11/calpactin binding proteinS100A10S100-A10, also known as p11, is a protein that is encoded by the S100A10 gene in humans and the S100a10 gene in other species. S100-A10 is a member of the S100 family of proteins containing two EF-hand calcium-binding motifs. S100 proteins are localized in the cytoplasm and/or nucleus of a wide...
and secretory leukoprotease inhibitor 1 (SLPISLPIAntileukoproteinase is an enzyme that in humans is encoded by the SLPI gene.-Further reading:* Victor E. Reviglio, Andres Grenat, Federico Pegoraro, Ruben H. Sambuelli, Tayyib Rana, and Irene C. Kuo. Secretory Leukoprotease Inhibitor: A Native Antimicrobial Protein in the Innate Immune Response in...
) - increased gluconeogenesisGluconeogenesisGluconeogenesis is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and glucogenic amino acids....
– glucose-6-phosphatase and tyrosine aminotransferaseTyrosine aminotransferaseTyrosine aminotransferase is an enzyme present in the liver and catalyzes the conversion of tyrosine to 4-hydroxyphenylpyruvate. In humans, the tyrosine aminotransferase protein is encoded by the TAT gene...
Transrepression
The opposite mechanism is called transrepressionTransrepression
In the field of molecular biology, transrepression is a process whereby one protein represses the activity of a second protein through a protein-protein interaction...
. The activated hormone receptor
Hormone receptor
A hormone receptor is a receptor protein on the surface of a cell or in its interior that binds to a specific hormone. The hormone causes many changes to take place in the cell....
interacts with specific transcription factor
Transcription factor
In molecular biology and genetics, a transcription factor is a protein that binds to specific DNA sequences, thereby controlling the flow of genetic information from DNA to mRNA...
s (such as AP-1
AP-1 (transcription factor)
In the field of molecular biology, the activator protein 1 is a transcription factor which is a heterodimeric protein composed of proteins belonging to the c-Fos, c-Jun, ATF and JDP families. It regulates gene expression in response to a variety of stimuli, including cytokines, growth factors,...
and NF-κB) and prevents the transcription
Transcription (genetics)
Transcription is the process of creating a complementary RNA copy of a sequence of DNA. Both RNA and DNA are nucleic acids, which use base pairs of nucleotides as a complementary language that can be converted back and forth from DNA to RNA by the action of the correct enzymes...
of targeted genes. Glucocorticoids are able to prevent the transcription of pro-inflammatory
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
genes, including interleukin
Interleukin
Interleukins are a group of cytokines that were first seen to be expressed by white blood cells . The term interleukin derives from "as a means of communication", and "deriving from the fact that many of these proteins are produced by leukocytes and act on leukocytes"...
s IL-1B, IL-4
Interleukin 4
Interleukin-4, abbreviated IL-4, is a cytokine that induces differentiation of naive helper T cells to Th2 cells. Upon activation by IL-4, Th2 cells subsequently produce additional IL-4. The cell that initially produces IL-4, thus inducing Th0 differentiation, has not been identified, but recent...
, IL-5
Interleukin 5
Interleukin 5 or IL-5 is an interleukin produced by T helper-2 cells and mast cells. Its functions are to stimulate B cell growth and increase immunoglobulin secretion. It is also a key mediator in eosinophil activation. IL-5 is a 115-amino acid -long TH2 cytokine that is part of the...
, and IL-8
Interleukin 8
Interleukin-8 is a chemokine produced by macrophages and other cell types such as epithelial cells. It is also synthesized by endothelial cells, which store IL-8 in their storage vesicles, the Weibel-Palade bodies...
, chemokines, cytokines, GM-CSF, and TNFA
Tumor necrosis factor
Tumor necrosis factor is a cytokine involved in systemic inflammation and is a member of a group of cytokines that stimulate the acute phase reaction...
genes.
Dissociation
The ordinary glucocorticoids do not distinguish among transactivation and transrepression and influence both the "wanted" immune and the "unwanted" genes regulating the metabolic and cardiovascular functions. Intensive research is aimed at discovering selectively acting glucocorticoids that will be able to repress only the immune system.Genetically modified mice that express a modified GR incapable of DNA binding are still responsive to the antiinflammatory effects of glucocorticoids, while the stimulation of gluconeogenesis by glucocorticoids is blocked. This result strongly suggests that most of the desirable antiinflammatory effects are due to transrepression, while the undesirable metabolic effects arise from transactivation, a hypothesis also underlying the development of selective glucocorticoid receptor agonist
Selective glucocorticoid receptor agonist
A selective glucocorticoid receptor agonist , sometimes called a dissociated glucocorticoid receptor agonist , is a type of experimental drug that is designed to share many of the desirable anti-inflammatory and immunosuppressive properties of classical glucocorticoid drugs but with fewer side...
s.
Non-genomic
Glucocorticoids have been shown to exert a number of rapid actions that are independent of the regulations of gene transcription. Binding of corticosteroids to the glucocorticoid receptor (GR) stimulates phosphatidylinositol 3-kinasePhosphoinositide 3-kinase
Phosphatidylinositol 3-kinases are a family of enzymes involved in cellular functions such as cell growth, proliferation, differentiation, motility, survival and intracellular trafficking, which in turn are involved in cancer. In response to lipopolysaccharide, PI3K phosphorylates p65, inducing...
and protein kinase AKT
AKT
Akt, also known as Protein Kinase B , is a serine/threonine protein kinase that plays a key role in multiple cellular processes such as glucose metabolism, cell proliferation, apoptosis, transcription and cell migration.-Family members:...
, leading to endothelial nitric oxide synthase
Endothelial NOS
Endothelial NOS , also known as nitric oxide synthase 3 or constitutive NOS , is an enzyme that in humans is encoded by the NOS3 gene....
(eNOS) activation and nitric oxide
Nitric oxide
Nitric oxide, also known as nitrogen monoxide, is a diatomic molecule with chemical formula NO. It is a free radical and is an important intermediate in the chemical industry...
-dependent vasorelaxation. Membrane associated GR has been shown to mediate lymphocytolysis. In addition, some glucocorticoids have been shown to rapidly inhibit the release of the inflammatory prostaglandin PGE2
Dinoprostone
The naturally occurring prostaglandin E2 is known in medicine as dinoprostone. It has important effects in labour and also stimulates osteoblasts to release factors that stimulate bone resorption by osteoclasts...
and this effect is blocked by the glucocorticoid receptor antagonist mifepristone
Mifepristone
Mifepristone is a synthetic steroid compound used as a pharmaceutical. It is a progesterone receptor antagonist used as an abortifacient in the first months of pregnancy, and in smaller doses as an emergency contraceptive. During early trials, it was known as RU-38486 or simply RU-486, its...
(RU-486) and this effect is not affected by protein synthesis inhibitors. This data together suggests a non-genomic mechanism of action.
Glucocorticoid-induced neutrophilia
Acute or chronic administration of corticosteroids causes neutrophilia suggesting that the enhanced release of PMNs from the bone marrow is an important mechanism of the glucocorticoid-induced granulocytosis. An alternative mechanism for the granulocytosis induced by glucocorticoids is an influx of PMNs from the intravascular marginated PMN pools. The response is caused by a shift of cells from the marginal to the circulating pool; hence, it frequently is referred to as demargination.Some of the immunosuppressive effects of glucocorticoids are mediated by non-genomic signalling involving the glucocortiocid receptor (GR). A multi-protein complex composed of the unliganded glucocorticoid receptor, Hsp90
Hsp90
Hsp90 is a molecular chaperone and is one of the most abundant proteins expressed in cells. It is a member of the heat shock protein family, which is upregulated in response to stress...
, and the tyrosine kinases LCK
Lck
Lck is a protein that is found inside specialized cells of the immune system called lymphocytes. Lck is a tyrosine kinase, which phosphorylates tyrosine residues of certain proteins involved in the intracellular signaling pathways of these lymphocytes...
and FYN
FYN
Proto-oncogene tyrosine-protein kinase Fyn is an enzyme that in humans is encoded by the FYN gene.This gene is a member of the protein-tyrosine kinase oncogene family. It encodes a membrane-associated tyrosine kinase that has been implicated in the control of cell growth...
is recruited to the antigen
Antigen
An antigen is a foreign molecule that, when introduced into the body, triggers the production of an antibody by the immune system. The immune system will then kill or neutralize the antigen that is recognized as a foreign and potentially harmful invader. These invaders can be molecules such as...
activated T cell receptor
T cell receptor
The T cell receptor or TCR is a molecule found on the surface of T lymphocytes that is responsible for recognizing antigens bound to major histocompatibility complex molecules...
(TCR) in T cell
T cell
T cells or T lymphocytes belong to a group of white blood cells known as lymphocytes, and play a central role in cell-mediated immunity. They can be distinguished from other lymphocytes, such as B cells and natural killer cells , by the presence of a T cell receptor on the cell surface. They are...
s. This GR complex is necessary for TCR signalling. On binding of glucocorticoids to GR, this multi-protein complex dissociates blocking TCR signalling.
Pharmacology
A variety of synthetic glucocorticoids, some far more potent than cortisol, have been created for therapeutic use. They differ in the pharmacokineticsPharmacokinetics
Pharmacokinetics, sometimes abbreviated as PK, is a branch of pharmacology dedicated to the determination of the fate of substances administered externally to a living organism...
(absorption factor, half-life, volume of distribution, clearance) and in pharmacodynamics
Pharmacodynamics
Pharmacodynamics is the study of the biochemical and physiological effects of drugs on the body or on microorganisms or parasites within or on the body and the mechanisms of drug action and the relationship between drug concentration and effect...
(for example the capacity of mineralocorticoid
Mineralocorticoid
Mineralocorticoids are a class of steroid hormones characterised by their similarity to aldosterone and their influence on salt and water balances.-Physiology:...
activity: retention of sodium
Sodium
Sodium is a chemical element with the symbol Na and atomic number 11. It is a soft, silvery-white, highly reactive metal and is a member of the alkali metals; its only stable isotope is 23Na. It is an abundant element that exists in numerous minerals, most commonly as sodium chloride...
(Na+) and water; see also: renal physiology). Because they permeate the intestine
Intestine
In human anatomy, the intestine is the segment of the alimentary canal extending from the pyloric sphincter of the stomach to the anus and, in humans and other mammals, consists of two segments, the small intestine and the large intestine...
s easily, they are administered primarily per os (by mouth
Mouth
The mouth is the first portion of the alimentary canal that receives food andsaliva. The oral mucosa is the mucous membrane epithelium lining the inside of the mouth....
), but also by other methods, such as topical
Topical
In medicine, a topical medication is applied to body surfaces such as the skin or mucous membranes such as the vagina, anus, throat, eyes and ears.Many topical medications are epicutaneous, meaning that they are applied directly to the skin...
ly on skin
Skin
-Dermis:The dermis is the layer of skin beneath the epidermis that consists of connective tissue and cushions the body from stress and strain. The dermis is tightly connected to the epidermis by a basement membrane. It also harbors many Mechanoreceptors that provide the sense of touch and heat...
. More than 90 percent of them bind different plasma proteins, however with a different binding specificity. Endogenous glucocorticoids and some synthetic corticoids have high affinity to the protein transcortin
Transcortin
Transcortin, also corticosteroid-binding globulin or CBG, is officially called serpin peptidase inhibitor, clade A , member 6.It is an alpha-globulin.-Binding:...
(also called CBG, corticosteroid-binding globulin), whereas all of them bind albumin
Serum albumin
Serum albumin, often referred to simply as albumin is a protein that in humans is encoded by the ALB gene.Serum albumin is the most abundant plasma protein in mammals. Albumin is essential for maintaining the osmotic pressure needed for proper distribution of body fluids between intravascular...
. In the liver, they quickly metabolise by conjugation with a sulfate
Sulfate
In inorganic chemistry, a sulfate is a salt of sulfuric acid.-Chemical properties:...
or glucuronic acid
Glucuronic acid
Glucuronic acid is a carboxylic acid. Its structure is similar to that of glucose. However, glucuronic acid's sixth carbon is oxidized to a carboxylic acid...
, and are secreted in the urine
Urine
Urine is a typically sterile liquid by-product of the body that is secreted by the kidneys through a process called urination and excreted through the urethra. Cellular metabolism generates numerous by-products, many rich in nitrogen, that require elimination from the bloodstream...
.
Glucocorticoid potency, duration of effect, and overlapping mineralocorticoid potency varies. Cortisol (hydrocortisone) is the standard of comparison for glucocorticoid potency. Hydrocortisone is the name used for pharmaceutical preparations of cortisol. Data refer to oral dosing, except when mentioned. Oral potency may be less than parenteral potency because significant amounts (up to 50% in some cases) may not be absorbed from the intestine. Fludrocortisone, DOCA (Deoxycorticosterone acetate), and aldosterone are, by definition, not considered glucocorticoids, although they may have minor glucocorticoid potency, and are included in this table to provide perspective on mineralocorticoid potency.
| Name | Glucocorticoid potency | Mineralocorticoid potency | Duration of action (t1/2 in hours) |
| Hydrocortisone (Cortisol) | 1 | 1 | 8 |
| Cortisone acetate | 0.8 | 0.8 | oral 8, intramuscular 18+ |
| Prednisone Prednisone Prednisone is a synthetic corticosteroid drug that is particularly effective as an immunosuppressant drug. It is used to treat certain inflammatory diseases and some types of cancer, but has significant adverse effects... |
3.5-5 | 0.8 | 16-36 |
| Prednisolone Prednisolone Prednisolone is the active metabolite of prednisone, which is also used as a drug.-Uses:Prednisolone is a corticosteroid drug with predominant glucocorticoid and low mineralocorticoid activity, making it useful for the treatment of a wide range of inflammatory and auto-immune conditions such as... |
4 | 0.8 | 16-36 |
| Methylprednisolone Methylprednisolone Methylprednisolone is a synthetic glucocorticoid or corticosteroid drug. It is marketed in the USA and Canada under the brand names Medrol and Solu-Medrol. It is also available as a generic drug.... |
5-7.5 | 0.5 | 18-40 |
| Dexamethasone Dexamethasone Dexamethasone is a potent synthetic member of the glucocorticoid class of steroid drugs. It acts as an anti-inflammatory and immunosuppressant... |
25-80 | 0 | 36-54 |
| Betamethasone Betamethasone Betamethasone is a potent glucocorticoid steroid with anti-inflammatory and immunosuppressive properties. Unlike other drugs with these effects, betamethasone does not cause water retention. It is applied as a topical cream, ointment, foam, lotion or gel to treat itching... |
25-30 | 0 | 36-54 |
| Triamcinolone Triamcinolone acetonide Triamcinolone acetonide is a synthetic corticosteroid used to treat various skin conditions and to relieve the discomfort of mouth sores. It is a more potent type of triamcinolone, being about 8 times as effective as prednisone.-Medical use:... |
5 | 0 | 12-36 |
| Beclometasone | 8 puffs 4 times a day equals 14 mg oral prednisone once a day |
- | - |
| Fludrocortisone Fludrocortisone Fludrocortisone is a synthetic corticosteroid with moderate glucocorticoid potency and much greater mineralocorticoid potency. The brand name in the U.S. and Canada is Florinef.-Uses:... acetate |
15 | 200 | 24 |
| Deoxycorticosterone Deoxycorticosterone 11-Deoxycorticosterone is a steroid hormone produced by the adrenal gland that possesses mineralocorticoid activity and acts as a precursor to aldosterone. As its names indicate, it can be understood as 21-hydroxy- variant of progesterone or a 11-deoxy- variant of corticosterone... acetate (DOCA) |
0 | 20 | - |
| Aldosterone Aldosterone Aldosterone is a hormone that increases the reabsorption of sodium ions and water and the release of potassium in the collecting ducts and distal convoluted tubule of the kidneys' functional unit, the nephron. This increases blood volume and, therefore, increases blood pressure. Drugs that... |
0.3 | 200-1000 | - |
Therapeutic use
Glucocorticoids may be used in low doses in adrenal insufficiencyAdrenal insufficiency
Adrenal insufficiency is a condition in which the adrenal glands, located above the kidneys, do not produce adequate amounts of steroid hormones , primarily cortisol, but may also include impaired aldosterone production which regulates sodium, potassium and water retention...
. In much higher doses, oral or inhaled glucocorticoids are used to suppress various allergic
Allergy
An Allergy is a hypersensitivity disorder of the immune system. Allergic reactions occur when a person's immune system reacts to normally harmless substances in the environment. A substance that causes a reaction is called an allergen. These reactions are acquired, predictable, and rapid...
, inflammatory
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
, and autoimmune disorders. Inhaled glucocorticoids are the second-line treatment for asthma
Asthma
Asthma is the common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm. Symptoms include wheezing, coughing, chest tightness, and shortness of breath...
. They are also administered as posttransplantory immunosuppressants to prevent the acute transplant rejection
Transplant rejection
Transplant rejection occurs when transplanted tissue is rejected by the recipient's immune system, which destroys the transplanted tissue. Transplant rejection can be lessened by determining the molecular similitude between donor and recipient and by use of immunosuppressant drugs after...
and the graft-versus-host disease
Graft-versus-host disease
Graft-versus-host disease is a common complication after a stem cell transplant or bone marrow transplant from another person . Immune cells in the donated marrow or stem cells recognize the recipient as "foreign". The transplanted immune cells then attack the host's body cells...
. Nevertheless, they do not prevent an infection and also inhibit later reparative processes.
Physiological replacement
Any glucocorticoid can be given in a dose that provides approximately the same glucocorticoid effects as normal cortisol production; this is referred to as physiologic, replacement, or maintenance dosing. This is approximately 6–12 mg/m²/day (m² refers to body surface areaBody surface area
In physiology and medicine, the body surface area is the measured or calculated surface of a human body. For many clinical purposes BSA is a better indicator of metabolic mass than body weight because it is less affected by abnormal adipose mass...
(BSA), and is a measure of body size; an average man is 1.7 m²).
Therapeutic immunosuppression
Glucocorticoids cause immunosuppressionImmunosuppression
Immunosuppression involves an act that reduces the activation or efficacy of the immune system. Some portions of the immune system itself have immuno-suppressive effects on other parts of the immune system, and immunosuppression may occur as an adverse reaction to treatment of other...
, and the therapeutic component of this effect is mainly the decreases in the the function and numbers of lymphocyte
Lymphocyte
A lymphocyte is a type of white blood cell in the vertebrate immune system.Under the microscope, lymphocytes can be divided into large lymphocytes and small lymphocytes. Large granular lymphocytes include natural killer cells...
s, including both B cell
B cell
B cells are lymphocytes that play a large role in the humoral immune response . The principal functions of B cells are to make antibodies against antigens, perform the role of antigen-presenting cells and eventually develop into memory B cells after activation by antigen interaction...
s and T cell
T cell
T cells or T lymphocytes belong to a group of white blood cells known as lymphocytes, and play a central role in cell-mediated immunity. They can be distinguished from other lymphocytes, such as B cells and natural killer cells , by the presence of a T cell receptor on the cell surface. They are...
s.
Glucocorticoids suppress the cell-mediated immunity
Cell-mediated immunity
Cell-mediated immunity is an immune response that does not involve antibodies but rather involves the activation of macrophages, natural killer cells , antigen-specific cytotoxic T-lymphocytes, and the release of various cytokines in response to an antigen...
. They act by inhibiting genes that code for the cytokines IL-1, IL-2
Interleukin 2
Interleukin-2 is an interleukin, a type of cytokine immune system signaling molecule, which is a leukocytotrophic hormone that is instrumental in the body's natural response to microbial infection and in discriminating between foreign and self...
, IL-3
Interleukin 3
Interleukin 3, also known as IL-3, is a protein that in humans is encoded by the IL3 gene.-Function:Interleukin-3 is an interleukin, a type of biological signal that can improve the body's natural response to disease as part of the immune system...
, IL-4
Interleukin 4
Interleukin-4, abbreviated IL-4, is a cytokine that induces differentiation of naive helper T cells to Th2 cells. Upon activation by IL-4, Th2 cells subsequently produce additional IL-4. The cell that initially produces IL-4, thus inducing Th0 differentiation, has not been identified, but recent...
, IL-5
Interleukin 5
Interleukin 5 or IL-5 is an interleukin produced by T helper-2 cells and mast cells. Its functions are to stimulate B cell growth and increase immunoglobulin secretion. It is also a key mediator in eosinophil activation. IL-5 is a 115-amino acid -long TH2 cytokine that is part of the...
, IL-6
Interleukin 6
Interleukin-6 is a protein that in humans is encoded by the IL6 gene.IL-6 is an interleukin that acts as both a pro-inflammatory and anti-inflammatory cytokine. It is secreted by T cells and macrophages to stimulate immune response, e.g. during infection and after trauma, especially burns or other...
, IL-8
Interleukin 8
Interleukin-8 is a chemokine produced by macrophages and other cell types such as epithelial cells. It is also synthesized by endothelial cells, which store IL-8 in their storage vesicles, the Weibel-Palade bodies...
and IFN-γ, the most important of which is IL-2. Smaller cytokine
Cytokine
Cytokines are small cell-signaling protein molecules that are secreted by the glial cells of the nervous system and by numerous cells of the immune system and are a category of signaling molecules used extensively in intercellular communication...
production reduces the T cell
T cell
T cells or T lymphocytes belong to a group of white blood cells known as lymphocytes, and play a central role in cell-mediated immunity. They can be distinguished from other lymphocytes, such as B cells and natural killer cells , by the presence of a T cell receptor on the cell surface. They are...
proliferation.
Glucocorticoids do, however, not only reduce T cell proliferation, but also lead to another well known effect called glucocorticoid induced apoptosis. The effect is more prominent in immature T cells that still reside in the thymus, but also affect peripheral T cells. The exact mechanism underlying this glucocorticoid sensitivity still remains to be elucidated.
Glucocorticoids also suppress the humoral immunity
Humoral immunity
The Humoral Immune Response is the aspect of immunity that is mediated by secreted antibodies produced in the cells of the B lymphocyte lineage . B Cells transform into plasma cells which secrete antibodies...
, thereby causing a humoral immune deficiency
Humoral immune deficiency
Humoral immune deficiencies are conditions which cause impairment of humoral immunity, which can lead to immunodeficiency. It can be mediated by insufficient number or function of B cells, the plasma cells they differentiate into , or the antibody secreted by the plasma cells.They are associated...
. Glucocorticoids cause B cell
B cell
B cells are lymphocytes that play a large role in the humoral immune response . The principal functions of B cells are to make antibodies against antigens, perform the role of antigen-presenting cells and eventually develop into memory B cells after activation by antigen interaction...
s to express smaller amounts of IL-2 and of IL-2 receptors. This diminishes both B cell clone expansion and antibody
Antibody
An antibody, also known as an immunoglobulin, is a large Y-shaped protein used by the immune system to identify and neutralize foreign objects such as bacteria and viruses. The antibody recognizes a unique part of the foreign target, termed an antigen...
synthesis. The diminished amounts of IL-2 also causes fewer T lymphocyte cells to be activated.
Since glucocorticoid is a steroid
Steroid
A steroid is a type of organic compound that contains a characteristic arrangement of four cycloalkane rings that are joined to each other. Examples of steroids include the dietary fat cholesterol, the sex hormones estradiol and testosterone, and the anti-inflammatory drug dexamethasone.The core...
, it regulates transcription factors; another factor it down-regulates is the expression of Fc receptor
Fc receptor
An Fc receptor is a protein found on the surface of certain cells - including natural killer cells, macrophages, neutrophils, and mast cells - that contribute to the protective functions of the immune system....
s on macrophage
Macrophage
Macrophages are cells produced by the differentiation of monocytes in tissues. Human macrophages are about in diameter. Monocytes and macrophages are phagocytes. Macrophages function in both non-specific defense as well as help initiate specific defense mechanisms of vertebrate animals...
s, so there is a decreased phagocytosis of opsonised
Opsonin
An opsonin is any molecule that targets an antigen for an immune response. However, the term is usually used in reference to molecules that act as a binding enhancer for the process of phagocytosis, especially antibodies, which coat the negatively-charged molecules on the membrane. Molecules that...
cells.
Anti-inflammatory
Glucocorticoids are potent anti-inflammatories, regardless of the inflammation's cause. Glucocorticoids' primary anti-inflammatory mechanism is lipocortin-1 (annexin-1) synthesis. Lipocortin-1 both suppresses phospholipase A2Phospholipase A2
Phospholipases A2 are enzymes that release fatty acids from the second carbon group of glycerol. This particular phospholipase specifically recognizes the sn-2 acyl bond of phospholipids and catalytically hydrolyzes the bond releasing arachidonic acid and lysophospholipids...
, thereby blocking eicosanoid
Eicosanoid
In biochemistry, eicosanoids are signaling molecules made by oxidation of twenty-carbon essential fatty acids, ....
production, and inhibits various leukocyte inflammatory events (epithelial
Epithelium
Epithelium is one of the four basic types of animal tissue, along with connective tissue, muscle tissue and nervous tissue. Epithelial tissues line the cavities and surfaces of structures throughout the body, and also form many glands. Functions of epithelial cells include secretion, selective...
adhesion
Cell adhesion
Cellular adhesion is the binding of a cell to a surface, extracellular matrix or another cell using cell adhesion molecules such as selectins, integrins, and cadherins. Correct cellular adhesion is essential in maintaining multicellular structure...
, emigration
Emigration
Emigration is the act of leaving one's country or region to settle in another. It is the same as immigration but from the perspective of the country of origin. Human movement before the establishment of political boundaries or within one state is termed migration. There are many reasons why people...
, chemotaxis
Chemotaxis
Chemotaxis is the phenomenon in which somatic cells, bacteria, and other single-cell or multicellular organisms direct their movements according to certain chemicals in their environment. This is important for bacteria to find food by swimming towards the highest concentration of food molecules,...
, phagocytosis, respiratory burst
Respiratory burst
Respiratory burst is the rapid release of reactive oxygen species from different types of cells....
, etc.). In other words, Glucocorticoids not only suppress immune response, but also inhibit the two main products of inflammation, prostaglandins and leukotrienes. Glucocorticoids inhibit prostaglandin synthesis at the level of phospholipase A2
Phospholipase A2
Phospholipases A2 are enzymes that release fatty acids from the second carbon group of glycerol. This particular phospholipase specifically recognizes the sn-2 acyl bond of phospholipids and catalytically hydrolyzes the bond releasing arachidonic acid and lysophospholipids...
as well as at the level of cyclooxygenase
Cyclooxygenase
Cyclooxygenase is an enzyme that is responsible for formation of important biological mediators called prostanoids, including prostaglandins, prostacyclin and thromboxane. Pharmacological inhibition of COX can provide relief from the symptoms of inflammation and pain...
/PGE isomerase (COX-1 and COX-2), the latter effect being much like that of NSAIDs
Non-steroidal anti-inflammatory drug
Nonsteroidal anti-inflammatory drugs, usually abbreviated to NSAIDs or NAIDs, but also referred to as nonsteroidal anti-inflammatory agents/analgesics or nonsteroidal Anti-inflammatory medicines , are drugs with analgesic and antipyretic effects and which have, in higher doses, anti-inflammatory...
, potentiating the anti-inflammatory effect.
In addition, glucocorticoids also suppress cyclooxygenase
Cyclooxygenase
Cyclooxygenase is an enzyme that is responsible for formation of important biological mediators called prostanoids, including prostaglandins, prostacyclin and thromboxane. Pharmacological inhibition of COX can provide relief from the symptoms of inflammation and pain...
expression.
Glucocorticoids marketed as anti-inflammatories are often topical formulations, such as nasal sprays for rhinitis
Rhinitis
Rhinitis , commonly known as a stuffy nose, is the medical term describing irritation and inflammation of some internal areas of the nose. The primary symptom of rhinitis is nasal dripping. It is caused by chronic or acute inflammation of the mucous membrane of the nose due to viruses, bacteria or...
or inhalers for asthma
Asthma
Asthma is the common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm. Symptoms include wheezing, coughing, chest tightness, and shortness of breath...
. These preparations have the advantage of only affecting the targeted area, thereby reducing side effects or potential interactions. In this case, the main compounds used are beclometasone, budesonide
Budesonide
Budesonide is a glucocorticoid steroid for the treatment of asthma and non-infectious rhinitis , and for treatment and prevention of nasal polyposis...
, fluticasone
Fluticasone
Fluticasone is a synthetic glucocorticoid.Both the furoate and propionate forms are used as topical anti-inflammatories:*Fluticasone propionate*Fluticasone furoateTreatment of asthma - Fluticasone in combination with Salmeterol - "[]" - aerosol....
, mometasone and ciclesonide
Ciclesonide
Ciclesonide is a glucocorticoid used to treat obstructive airway diseases. It is marketed under the brand name Alvesco for asthma and Omnaris/Omniair for hayfever in the US & Canada...
. In rhinitis, sprays are used. For asthma, glucocorticoids are administered as inhalant
Inhalant
Inhalants are a broad range of drugs whose volatile vapors are taken in via the nose and trachea. They are taken by volatilization, and do not include drugs that are inhaled after burning or heating...
s with a metered-dose or dry powder inhaler
Dry powder inhaler
A Dry powder inhaler is a device that delivers medication to the lungs in the form of a dry powder. DPIs are commonly used to treat respiratory diseases such as asthma, bronchitis, emphysema and COPD although DPIs have also been used in the treatment of diabetes mellitus.DPIs are an alternative...
.
Hyperaldosteronism
Glucocorticoids can be used in the management of familial hyperaldosteronism type 1. They are not effective however, for use in the type 2 condition.Resistance
Resistance to the therapeutic uses of glucocorticoids can present difficulty; for instance, 25% of cases of severe asthmaAsthma
Asthma is the common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm. Symptoms include wheezing, coughing, chest tightness, and shortness of breath...
may be unresponsive to steroids. This may be the result of genetic predisposition, ongoing exposure to the cause of the inflammation (such as allergen
Allergen
An allergen is any substance that can cause an allergy. In technical terms, an allergen is a non-parasitic antigen capable of stimulating a type-I hypersensitivity reaction in atopic individuals....
s), immunological phenomena that bypass glucocorticoids, and pharmacokinetic disturbances (incomplete absorption or accelerated excretion or metabolism).
Side-effects
Glucocorticoid drugs currently being used act nonselectively, so in the long run they may impair many healthy anabolic processes. To prevent this, much research has been focused recently on the elaboration of selectively acting glucocorticoid drugs. These are the side-effects that could be prevented:- immunodeficiency (see separate section below)
- hyperglycemiaHyperglycemiaHyperglycemia or Hyperglycæmia, or high blood sugar, is a condition in which an excessive amount of glucose circulates in the blood plasma. This is generally a glucose level higher than 13.5mmol/l , but symptoms may not start to become noticeable until even higher values such as 15-20 mmol/l...
due to increased gluconeogenesisGluconeogenesisGluconeogenesis is a metabolic pathway that results in the generation of glucose from non-carbohydrate carbon substrates such as lactate, glycerol, and glucogenic amino acids....
, insulin resistanceInsulin resistanceInsulin resistance is a physiological condition where the natural hormone insulin becomes less effective at lowering blood sugars. The resulting increase in blood glucose may raise levels outside the normal range and cause adverse health effects, depending on dietary conditions. Certain cell types...
, and impaired glucose tolerance ("steroid diabetesSteroid diabetesSteroid diabetes is a medical term referring to prolonged hyperglycemia due to glucocorticoid therapy for another medical condition...
"); caution in those with diabetes mellitusDiabetes mellitusDiabetes mellitus, often simply referred to as diabetes, is a group of metabolic diseases in which a person has high blood sugar, either because the body does not produce enough insulin, or because cells do not respond to the insulin that is produced... - increased skinSkin-Dermis:The dermis is the layer of skin beneath the epidermis that consists of connective tissue and cushions the body from stress and strain. The dermis is tightly connected to the epidermis by a basement membrane. It also harbors many Mechanoreceptors that provide the sense of touch and heat...
fragility, easy bruisingBruiseA bruise, also called a contusion, is a type of relatively minor hematoma of tissue in which capillaries and sometimes venules are damaged by trauma, allowing blood to seep into the surrounding interstitial tissues. Bruises can involve capillaries at the level of skin, subcutaneous tissue, muscle,... - negative calcium balance due to reduced intestinal calcium absorption
- Steroid-induced osteoporosisSteroid-induced osteoporosisSteroid-induced osteoporosis is osteoporosis arising due to use of glucocorticoids - analogous to Cushing's syndrome and involving mainly the axial skeleton. The synthetic glucocorticoid prescription drug prednisone is a main candidate after prolonged intake...
: reduced boneBoneBones are rigid organs that constitute part of the endoskeleton of vertebrates. They support, and protect the various organs of the body, produce red and white blood cells and store minerals. Bone tissue is a type of dense connective tissue...
density (osteoporosisOsteoporosisOsteoporosis is a disease of bones that leads to an increased risk of fracture. In osteoporosis the bone mineral density is reduced, bone microarchitecture is deteriorating, and the amount and variety of proteins in bone is altered...
, osteonecrosis, higher fracture risk, slower fracture repair) - weight gain due to increased visceral and truncal fatAdipose tissueIn histology, adipose tissue or body fat or fat depot or just fat is loose connective tissue composed of adipocytes. It is technically composed of roughly only 80% fat; fat in its solitary state exists in the liver and muscles. Adipose tissue is derived from lipoblasts...
deposition (central obesityCentral obesityAbdominal obesity, colloquially known as belly fat or clinically as central obesity, is the accumulation of abdominal fat resulting in an increase in waist size...
) and appetiteAppetiteThe appetite is the desire to eat food, felt as hunger. Appetite exists in all higher life-forms, and serves to regulate adequate energy intake to maintain metabolic needs. It is regulated by a close interplay between the digestive tract, adipose tissue and the brain. Decreased desire to eat is...
stimulation - adrenal insufficiencyAdrenal insufficiencyAdrenal insufficiency is a condition in which the adrenal glands, located above the kidneys, do not produce adequate amounts of steroid hormones , primarily cortisol, but may also include impaired aldosterone production which regulates sodium, potassium and water retention...
(if used for long time and stopped suddenly without a taper) - muscleMuscleMuscle is a contractile tissue of animals and is derived from the mesodermal layer of embryonic germ cells. Muscle cells contain contractile filaments that move past each other and change the size of the cell. They are classified as skeletal, cardiac, or smooth muscles. Their function is to...
breakdown (proteolysis), weakness; reduced muscle mass and repair - expansion of malar fat pads and dilation of small blood vesselBlood vesselThe blood vessels are the part of the circulatory system that transports blood throughout the body. There are three major types of blood vessels: the arteries, which carry the blood away from the heart; the capillaries, which enable the actual exchange of water and chemicals between the blood and...
s in skin - anovulationAnovulationAn anovulatory cycle is a menstrual cycle during which the ovaries do not release an oocyte. Therefore, ovulation does not take place. However, a woman who does not ovulate at each menstrual cycle is not necessarily going through menopause...
, irregularity of menstrual periodsMenstrual cycleThe menstrual cycle is the scientific term for the physiological changes that can occur in fertile women for the purpose of sexual reproduction. This article focuses on the human menstrual cycle.... - growth failure, pubertal delayDelayed pubertyPuberty is described as delayed puberty with exceptions when an organism has passed the usual age of onset of puberty with no physical or hormonal signs that it is beginning. Puberty may be delayed for several years and still occur normally, in which case it is considered constitutional delay, a...
- increased plasma amino acidAmino acidAmino acids are molecules containing an amine group, a carboxylic acid group and a side-chain that varies between different amino acids. The key elements of an amino acid are carbon, hydrogen, oxygen, and nitrogen...
s, increased ureaUreaUrea or carbamide is an organic compound with the chemical formula CO2. The molecule has two —NH2 groups joined by a carbonyl functional group....
formation; negative nitrogen balance - excitatory effect on central nervous systemCentral nervous systemThe central nervous system is the part of the nervous system that integrates the information that it receives from, and coordinates the activity of, all parts of the bodies of bilaterian animals—that is, all multicellular animals except sponges and radially symmetric animals such as jellyfish...
(euphoria, psychosis) - glaucomaGlaucomaGlaucoma is an eye disorder in which the optic nerve suffers damage, permanently damaging vision in the affected eye and progressing to complete blindness if untreated. It is often, but not always, associated with increased pressure of the fluid in the eye...
due to increased cranial pressure - cataracts
In high doses, hydrocortisone (cortisol) and those glucocorticoids with appreciable mineralocorticoid potency can exert a mineralocorticoid effect as well, although in physiologic doses this is prevented by rapid degradation of cortisol by 11β-hydroxysteroid dehydrogenase isoenzyme 2 (11β-HSD2
Protein:HSD11B2
Corticosteroid 11-β-dehydrogenase isozyme 2 also known as 11-β-hydroxysteroid dehydrogenase 2 is an enzyme that in humans is encoded by the HSD11B2 gene.- Function :...
) in mineralocorticoid target tissues. Mineralocorticoid effects can include salt and water retention, extracellular fluid
Extracellular fluid
Extracellular fluid usually denotes all body fluid outside of cells. The remainder is called intracellular fluid.In some animals, including mammals, the extracellular fluid can be divided into two major subcompartments, interstitial fluid and blood plasma...
volume expansion, hypertension
Hypertension
Hypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
, potassium
Potassium
Potassium is the chemical element with the symbol K and atomic number 19. Elemental potassium is a soft silvery-white alkali metal that oxidizes rapidly in air and is very reactive with water, generating sufficient heat to ignite the hydrogen emitted in the reaction.Potassium and sodium are...
depletion, and metabolic alkalosis
Metabolic alkalosis
Metabolic alkalosis is a metabolic condition in which the pH of tissue is elevated beyond the normal range . This is the result of decreased hydrogen ion concentration, leading to increased bicarbonate, or alternatively a direct result of increased bicarbonate concentrations.-Terminology:*Alkalosis...
.
The combination of clinical problems produced by prolonged, excess glucocorticoids, whether synthetic or endogenous, is termed Cushing's syndrome
Cushing's syndrome
Cushing's syndrome is a hormone disorder caused by high levels of cortisol in the blood. This can be caused by taking glucocorticoid drugs, or by tumors that produce cortisol or adrenocorticotropic hormone or CRH...
.
Immunodeficiency
Glucocorticoids cause immunosuppressionImmunosuppression
Immunosuppression involves an act that reduces the activation or efficacy of the immune system. Some portions of the immune system itself have immuno-suppressive effects on other parts of the immune system, and immunosuppression may occur as an adverse reaction to treatment of other...
, decreasing the function and/or numbers of neutrophils, lymphocytes (including both B cell
B cell
B cells are lymphocytes that play a large role in the humoral immune response . The principal functions of B cells are to make antibodies against antigens, perform the role of antigen-presenting cells and eventually develop into memory B cells after activation by antigen interaction...
s and T cell
T cell
T cells or T lymphocytes belong to a group of white blood cells known as lymphocytes, and play a central role in cell-mediated immunity. They can be distinguished from other lymphocytes, such as B cells and natural killer cells , by the presence of a T cell receptor on the cell surface. They are...
s, monocyte
Monocyte
Monocytes are a type of white blood cell and are part of the innate immune system of vertebrates including all mammals , birds, reptiles, and fish. Monocytes play multiple roles in immune function...
s, macrophage
Macrophage
Macrophages are cells produced by the differentiation of monocytes in tissues. Human macrophages are about in diameter. Monocytes and macrophages are phagocytes. Macrophages function in both non-specific defense as well as help initiate specific defense mechanisms of vertebrate animals...
s, and the anatomical barrier function of the skin. This suppression, if large enough, cause manifestations of immunodeficiency
Immunodeficiency
Immunodeficiency is a state in which the immune system's ability to fight infectious disease is compromised or entirely absent. Immunodeficiency may also decrease cancer immunosurveillance. Most cases of immunodeficiency are acquired but some people are born with defects in their immune system,...
, including ones of T cell deficiency
T cell deficiency
T cell deficiency is a deficiency of T cells, either caused by lymphocytopenia of T cells or by decreased function of individual T cells. It causes an immunodeficiency of cell-mediated immunity.-By complete versus partial deficiency:...
, humoral immune deficiency
Humoral immune deficiency
Humoral immune deficiencies are conditions which cause impairment of humoral immunity, which can lead to immunodeficiency. It can be mediated by insufficient number or function of B cells, the plasma cells they differentiate into , or the antibody secreted by the plasma cells.They are associated...
as well as neutropenia
Neutropenia
Neutropenia, from Latin prefix neutro- and Greek suffix -πενία , is a granulocyte disorder characterized by an abnormally low number of neutrophils, the most important type of white blood cell...
.
| Bacteria Pathogenic bacteria Pathogenic bacteria are bacteria that cause bacterial infection. This article deals with human pathogenic bacteria.Although the vast majority of bacteria are harmless or beneficial, quite a few bacteria are pathogenic... |
|
|---|---|
| Fungi |
Aspergillus Aspergillus is a genus consisting of several hundred mold species found in various climates worldwide. Aspergillus was first catalogued in 1729 by the Italian priest and biologist Pier Antonio Micheli... Blastomyces Blastomyces is a fungal genus responsible for the medical condition blastomycosis.The most well known species of the genus is Blastomyces dermatitidis. B. dermatitidis is a dimorphic fungal pathogen, found primarily in the Mid-West and Northern United States and Canada... Candida albicans Candida albicans is a diploid fungus that grows both as yeast and filamentous cells and a causal agent of opportunistic oral and genital infections in humans. Systemic fungal infections including those by C... and nonalbicans species Coccidioides immitis Coccidioides immitis is a pathogenic fungus that resides in the soil in certain parts of the southwestern United States, northern Mexico, and a few other areas in the Western Hemisphere.... Cryptococcus neoformans Cryptococcus neoformans is an encapsulated yeast that can live in both plants and animals. Its teleomorph is Filobasidiella neoformans, a filamentous fungus belonging to the class Tremellomycetes. It is often found in pigeon excrement.... Fusarium Fusarium is a large genus of filamentous fungi widely distributed in soil and in association with plants. Most species are harmless saprobes, and are relatively abundant members of the soil microbial community. Some species produce mycotoxins in cereal crops that can affect human and animal health... species Penicillium marneffei Penicillium species are usually regarded as unimportant in terms of causing human disease. Penicillium marneffei, discovered in 1956, is different... |
| Viruses |
Cytomegalovirus Cytomegalovirus is a viral genus of the viral group known as Herpesviridae or herpesviruses. It is typically abbreviated as CMV: The species that infects humans is commonly known as human CMV or human herpesvirus-5 , and is the most studied of all cytomegaloviruses... Herpes simplex virus Herpes simplex virus 1 and 2 , also known as Human herpes virus 1 and 2 , are two members of the herpes virus family, Herpesviridae, that infect humans. Both HSV-1 and HSV-2 are ubiquitous and contagious... Human papillomavirus Human papillomavirus is a member of the papillomavirus family of viruses that is capable of infecting humans. Like all papillomaviruses, HPVs establish productive infections only in keratinocytes of the skin or mucous membranes... Influenza Influenza, commonly referred to as the flu, is an infectious disease caused by RNA viruses of the family Orthomyxoviridae , that affects birds and mammals... /parainfluenza |
| Other |
Cryptosporidiosis Cryptosporidiosis, also known as crypto, is a parasitic disease caused by Cryptosporidium, a protozoan parasite in the phylum Apicomplexa. It affects the intestines of mammals and is typically an acute short-term infection... /lsospora belli Strongyloides stercoralis Strongyloides stercoralis, also known as the threadworm, is the scientific name of a human parasitic roundworm causing the disease of strongyloidiasis.... Toxoplasma gondii Toxoplasma gondii is a species of parasitic protozoa in the genus Toxoplasma. The definitive host of T. gondii is the cat, but the parasite can be carried by many warm-blooded animals . Toxoplasmosis, the disease of which T... |
Withdrawal
In addition to the effects listed above, use of high-dose steroids for more than a week begins to produce suppression of the patient's adrenal glands because the exogenous glucocorticoids suppress hypothalamic corticotropin-releasing hormoneCorticotropin-releasing hormone
Corticotropin-releasing hormone , originally named corticotropin-releasing factor , and also called corticoliberin, is a polypeptide hormone and neurotransmitter involved in the stress response...
(CRH) and pituitary adrenocorticotropic hormone
Adrenocorticotropic hormone
Adrenocorticotropic hormone , also known as 'corticotropin', 'Adrenocorticotrophic hormone', is a polypeptide tropic hormone produced and secreted by the anterior pituitary gland. It is an important component of the hypothalamic-pituitary-adrenal axis and is often produced in response to biological...
(ACTH). With prolonged suppression, the adrenal glands atrophy (physically shrink), and can take months to recover full function after discontinuation of the exogenous glucocorticoid.
During this recovery time, the patient is vulnerable to adrenal insufficiency
Adrenal insufficiency
Adrenal insufficiency is a condition in which the adrenal glands, located above the kidneys, do not produce adequate amounts of steroid hormones , primarily cortisol, but may also include impaired aldosterone production which regulates sodium, potassium and water retention...
during times of stress, such as illness. While there is wide individual variation in suppressive dose and time for adrenal recovery, clinical guidelines have been devised to estimate potential adrenal suppression and recovery, to reduce risk to the patient. The following is one example, but many variations exist or may be appropriate in individual circumstances.
- If a patient has been receiving daily high doses for 5 days or less, they can be abruptly stopped (or reduced to physiologic replacement if patient is adrenal-deficient). Full adrenal recovery can be assumed to occur by a week afterward.
- If high doses were used for 6–10 days, reduce to replacement dose immediately and taper over 4 more days. Adrenal recovery can be assumed to occur within 2–4 weeks of completion of steroids.
- If high doses were used for 11–30 days, cut immediately to twice replacement, and then by 25% every 4 days. Stop entirely when dose is less than half of replacement. Full adrenal recovery should occur within 1–3 months of completion of withdrawal.
- If high doses were used more than 30 days, cut dose immediately to twice replacement, and reduce by 25% each week until replacement is reached.
- Then change to oral hydrocortisone or cortisone as a single morning dose, and gradually decrease by 2.5 mg each week. When a.m. dose is less than replacement, the return of normal basal adrenal function may be documented by checking 0800 cortisol levels prior to the morning dose; stop drugs when 0800 cortisol is 10 μg/dl. It is difficult to predict the time to full adrenal recovery after prolonged suppressive exogenous steroids; some people may take nearly a year.
- Flare-up of the underlying condition for which steroids are given may require a more gradual taper than outlined above.
Chemical Synthesis
See also
- GITR (glucocorticoid-induced TNF receptor)
- Glucocorticoid receptorGlucocorticoid receptorThe glucocorticoid receptor also known as NR3C1 is the receptor to which cortisol and other glucocorticoids bind....
- Immunosuppressive drugImmunosuppressive drugImmunosuppressive drugs or immunosuppressive agents are drugs that inhibit or prevent activity of the immune system. They are used in immunosuppressive therapy to:...
- Selective glucocorticoid receptor agonistSelective glucocorticoid receptor agonistA selective glucocorticoid receptor agonist , sometimes called a dissociated glucocorticoid receptor agonist , is a type of experimental drug that is designed to share many of the desirable anti-inflammatory and immunosuppressive properties of classical glucocorticoid drugs but with fewer side...
(SEGRA) - Topical steroidTopical steroidTopical steroids are the topical forms of corticosteroids. Topical steroids are the most commonly prescribed topical medications for the treatment of rash, eczema, and dermatitis. Topical steroids have anti-inflammatory properties, and are classified based on their vasoconstriction abilities. There...