

Diabetes mellitus
Encyclopedia
Diabetes mellitus, often simply referred to as diabetes, is a group of metabolic diseases in which a person has high blood sugar
, either because the body does not produce enough insulin
, or because cells do not respond to the insulin that is produced. This high blood sugar produces the classical symptoms of polyuria
(frequent urination), polydipsia
(increased thirst) and polyphagia
(increased hunger).
There are three main types of diabetes:
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes
.
All forms of diabetes have been treatable since insulin
became available in 1921, and type 2 diabetes may be controlled with medications. Both type 1 and 2 are chronic
conditions that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery
has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycemia
, diabetic ketoacidosis
, or nonketotic hyperosmolar coma
. Serious long-term complications include cardiovascular disease
, chronic renal failure
, retinal damage
. Adequate treatment of diabetes is thus important, as well as blood pressure
control and lifestyle factors such as smoking
cessation and maintaining a healthy body weight.
As of 2000 at least 171 million people worldwide have diabetes, or 2.8% of the population. Type 2 diabetes is by far the most common, affecting 90 to 95% of the U.S. diabetes population.
, type 2
, and gestational diabetes
. A few other types are described. The term diabetes, without qualification, usually refers to diabetes mellitus. The rare disease diabetes insipidus
has similar symptoms as diabetes mellitus, but without disturbances in the sugar metabolism (insipidus meaning "without taste" in Latin).
The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and non-insulin-dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard nomenclature. Various sources have defined "type 3 diabetes" as: gestational diabetes
, insulin-resistant type 1 diabetes (or "double diabetes"), type 2 diabetes which has progressed to require injected insulin, and latent autoimmune diabetes
of adults (or LADA or "type 1.5
" diabetes).
s of the islets of Langerhans
in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune
attack. There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children.
"Brittle" diabetes, also known as unstable diabetes or labile diabetes, is a term that was traditionally used to describe to dramatic and recurrent swings in glucose
levels, often occurring for no apparent reason in insulin
-dependent diabetes. This term, however, has no biologic basis and should not be used. There are many different reasons for type 1 diabetes to be accompanied by irregular and unpredictable hyperglycemia
s, frequently with ketosis
, and sometimes serious hypoglycemia
s, including an impaired counterregulatory response to hypoglycemia, occult infection, gastroparesis (which leads to erratic absorption of dietary carbohydrates), and endocrinopathies (eg, Addison's disease). These phenomena are believed to occur no more frequently than in 1% to 2% of persons with type 1 diabetes.
which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor
. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications
that improve insulin sensitivity or reduce glucose production by the liver
.
and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant
production and cause respiratory distress syndrome
. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental function. A cesarean section
may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia
.
A 2008 study completed in the U.S. found that the number of American women entering pregnancy with preexisting diabetes is increasing. In fact the rate of diabetes in expectant mothers has more than doubled in the past 6 years. This is particularly problematic as diabetes raises the risk of complications during pregnancy, as well as increasing the potential that the children of diabetic mothers will also become diabetic in the future.
Many people destined to develop type 2 diabetes spend many years in a state of pre-diabetes which has been termed "America's largest healthcare epidemic."
Latent autoimmune diabetes of adults is a condition in which Type 1 diabetes develops in adults. Adults with LADA are frequently initially misdiagnosed as having Type 2 diabetes, based on age rather than etiology
.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon. Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell
function. Abnormal insulin action may also have been genetically determined in some cases. Any disease that causes extensive damage to the pancreas
may lead to diabetes (for example, chronic pancreatitis
and cystic fibrosis
). Diseases associated with excessive secretion of insulin-antagonistic
hormone
s can cause diabetes (which is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some toxins damage pancreatic beta cells. The ICD
-10 (1992) diagnostic entity, malnutrition-related diabetes mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization
when the current taxonomy was introduced in 1999.
(frequent urination), polydipsia
(increased thirst) and polyphagia
(increased hunger). Symptoms may develop rapidly (weeks or months) in type 1 diabetes while in type 2 diabetes they usually develop much more slowly and may be subtle or absent.
Prolonged high blood glucose causes glucose absorption, which leads to changes in the shape of the lenses of the eyes, resulting in vision changes; sustained sensible glucose control usually returns the lens to its original shape. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected .
, a state of metabolic dysregulation characterized by the smell of acetone
; a rapid, deep breathing known as Kussmaul breathing
; nausea; vomiting and abdominal pain
; and altered states of consciousness.
A rarer but equally severe possibility is hyperosmolar nonketotic state
, which is more common in type 2 diabetes and is mainly the result of dehydration. Often, the patient has been drinking extreme amounts of sugar-containing drinks, leading to a vicious circle
in regard to the water loss.
s.
Diabetes doubles the risk of cardiovascular disease
. The main "macrovascular" diseases
(related to atherosclerosis
of larger arteries) are ischemic heart disease (angina
and myocardial infarction
), stroke
and peripheral vascular disease.
Diabetes also causes "microvascular" complications—damage to the small blood vessels. Diabetic retinopathy
, which affects blood vessel formation in the retina
of the eye, can lead to visual symptoms, reduced vision, and potentially blindness
. Diabetic nephropathy
, the impact of diabetes on the kidneys, can lead to scarring changes in the kidney tissue
, loss of small
or progressively larger
amounts of protein in the urine, and eventually chronic kidney disease requiring dialysis
. Diabetic neuropathy
is the impact of diabetes on the nervous system
, most commonly causing numbness, tingling and pain in the feet and also increasing the risk of skin damage due to altered sensation. Together with vascular disease in the legs, neuropathy contributes to the risk of diabetes-related foot problems
(such as diabetic foot ulcers) that can be difficult to treat and occasionally require amputation
.
Type 1 diabetes is partly inherited and then triggered by certain infections, with some evidence pointing at Coxsackie B4 virus
. There is a genetic element in individual susceptibility to some of these triggers which has been traced to particular HLA
genotype
s (i.e., the genetic "self" identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 diabetes mellitus seems to require an environmental trigger.
Type 2 diabetes is due primarily to lifestyle factors and genetics.
Following is a comprehensive list of other causes of diabetes:
 Insulin is the principal hormone that regulates uptake of glucose
Insulin is the principal hormone that regulates uptake of glucose
from the blood into most cells (primarily muscle and fat cells, but not central nervous system cells). Therefore deficiency of insulin or the insensitivity of its receptors
plays a central role in all forms of diabetes mellitus.
Humans are capable of digesting some carbohydrates
, in particular those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms most notably the monosaccharide
glucose
, the principal carbohydrate energy source used by the body. The rest are passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-cells), found in the Islets of Langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen
for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the beta cells and in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon
which acts in the opposite manner to insulin. Glucose thus forcibly produced from internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export mechanism. Normally liver cells do this when the level of insulin is low (which normally correlates with low levels of blood glucose).
Higher insulin levels increase some anabolic
("building up") processes such as cell growth and duplication, protein synthesis
, and fat
storage. Insulin (or its lack) is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic
to an anabolic direction, and vice versa. In particular, a low insulin level is the trigger for entering or leaving ketosis (the fat burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or resistance
), or if the insulin itself is defective, then glucose will not have its usual effect so that glucose will not be absorbed properly by those body cells that require it nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis
.
When the glucose concentration in the blood is raised beyond its renal threshold
(about 10 mmol/L, although this may be altered in certain conditions, such as pregnancy), reabsorption
of glucose in the proximal renal tubuli
is incomplete, and part of the glucose remains in the urine
(glycosuria
). This increases the osmotic pressure
of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria
) and increased fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body compartments, causing dehydration
and increased thirst.
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. It is preferable to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test. According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
People with fasting glucose levels from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) are considered to have impaired fasting glucose. Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired glucose tolerance
. Of these two pre-diabetic states, the latter in particular is a major risk factor for progression to full-blown diabetes mellitus as well as cardiovascular disease.
Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and death from any cause.
Patient education, understanding, and participation is vital since the complications of diabetes are far less common and less severe in people who have well-managed blood sugar levels. The goal of treatment is an HbA1C level of 6.5%, but should not be lower than that, and may be set higher. Attention is also paid to other health problems that may accelerate the deleterious effects of diabetes. These include smoking
, elevated cholesterol
levels, obesity
, high blood pressure
, and lack of regular exercise.
Metformin
is generally recommended as a first line treatment for type 2 diabetes as there is good evidence that it decreases mortality. Routine use of aspirin
however has not been found to improve outcomes in uncomplicated diabetes.
Insulin
Type 1 diabetes is typically treated with a combinations of regular and NPH insulin
, or synthetic insulin analogs. When insulin
is used in type 2 diabetes, a long-acting formulation is usually added initially, while continuing oral medications. Doses of insulin are then increased to effect.
system, such as the United Kingdom
, care may take place mainly outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood sugar control, or research projects. In other circumstances, general practitioners and specialists share care of a patient in a team approach. Optometrists
, podiatrists
/chiropodists, dietitian
s, physiotherapists
, nursing specialists (e.g., DSNs (Diabetic Specialist Nurse)), nurse practitioner
s, or certified diabetes educator
s, may jointly provide multidisciplinary expertise.
Prevalence in the United States
For at least 20 years, diabetes rates in North America have been increasing substantially. In 2010 nearly 26 million people have diabetes in the United States alone, from those 7 million people remain undiagnosed. Another 57 million people are estimated to have pre-diabetes.
The Centers for Disease Control has termed the change an epidemic
. The National Diabetes Information Clearinghouse estimates that diabetes costs $132 billion in the United States alone every year. About 5%–10% of diabetes cases in North America are type 1, with the rest being type 2. The fraction of type 1 in other parts of the world differs. Most of this difference is not currently understood. The American Diabetes Association cite the 2003 assessment of the National Center for Chronic Disease Prevention and Health Promotion (Centers for Disease Control and Prevention) that 1 in 3 Americans born after 2000 will develop diabetes in their lifetime.
According to the American Diabetes Association, approximately 18.3% (8.6 million) of Americans age 60 and older have diabetes. Diabetes mellitus prevalence increases with age, and the numbers of older persons with diabetes are expected to grow as the elderly population increases in number. The National Health and Nutrition Examination Survey (NHANES III) demonstrated that, in the population over 65 years old, 18% to 20% have diabetes, with 40% having either diabetes or its precursor form of impaired glucose tolerance
.
Prevalence in Australia
Indigenous populations in first world countries have a higher prevalence and increasing incidence of diabetes than their corresponding non-indigenous populations. In Australia the age-standardised prevalence of self-reported diabetes in Indigenous Australians is almost 4 times that of non-indigenous Australians. Preventative community health programs such as Sugar Man (diabetes education)
are showing some success in tackling this problem.
diabētēs, which in turn comes from Ancient Greek
διαβήτης (diabētēs) which literally means “a passer through; a siphon
.” Ancient Greek
physician
Aretaeus of Cappadocia
(fl.
1st century CE
) used that word, with the intended meaning “excessive discharge of urine,” as the name for the disease. Ultimately, the word comes from Greek διαβαίνειν (diabainein), meaning “to pass through,” which is composed of δια- (dia-), meaning “through” and βαίνειν (bainein), meaning “to go”. The word “diabetes” is first recorded in English, in the form diabete, in a medical text written around 1425.
The word “mellitus” (m or ˈ) comes from the classical Latin word mellītus, meaning “mellite” (i.e. sweetened with honey; honey-sweet). The Latin word comes from mell-, which comes from mel, meaning “honey; sweetness; pleasant thing,” and the suffix -ītus, whose meaning is the same as that of the English suffix “-ite.” It was Thomas Willis
who in 1675 added “mellitus” to the word “diabetes” as a designation for the disease, when he noticed that the urine of a diabetic had a sweet taste (glycosuria
). This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians, Indians, and Persians.
1550 BCE
mentions the phrase “the passing of too much urine.” The great Indian physician Sushruta (fl.
6th century BCE
) identified the disease and classified it as Medhumeha. He further identified it with obesity
and sedentary lifestyle, advising exercises to help "cure" it. The ancient India
ns tested for diabetes by observing whether ant
s were attracted to a person's urine, and called the ailment "sweet urine disease" (Madhumeha).
Concerning the sweetness of urine, it is to be noted that the Chinese, Japanese and Korean words for diabetes are based on the same ideographs (糖尿病) which mean "sugar urine disease". It was in 1776 that Matthew Dobson confirmed that the sweet taste comes from an excess of a kind of sugar in the urine and blood.
The first complete clinical description of diabetes was given by the Ancient Greek
physician
Aretaeus of Cappadocia
(fl.
1st century CE
), who noted the excessive amount of urine which passed through the kidneys and gave the disease the name “diabetes.”
Diabetes mellitus appears to have been a death sentence in the ancient era. Hippocrates makes no mention of it, which may indicate that he felt the disease was incurable. Aretaeus did attempt to treat it but could not give a good prognosis; he commented that "life (with diabetes) is short, disgusting and painful."
In medieval Persia
, Avicenna
(980–1037) provided a detailed account on diabetes mellitus in The Canon of Medicine
, "describing the abnormal appetite and the collapse of sexual functions," and he documented the sweet taste of diabetic urine. Like Aretaeus before him, Avicenna recognized a primary and secondary diabetes. He also described diabetic gangrene
, and treated diabetes using a mixture of lupin
e, trigonella
(fenugreek
), and zedoary
seed, which produces a considerable reduction in the excretion of sugar, a treatment which is still prescribed in modern times. Avicenna also "described diabetes insipidus very precisely for the first time", though it was later Johann Peter Frank
(1745–1821) who first differentiated between diabetes mellitus and diabetes insipidus.
Although diabetes has been recognized since antiquity
, and treatments of various efficacy have been known in various regions since the Middle Ages
, and in legend
for much longer, pathogenesis of diabetes has only been understood experimentally since about 1900.
The discovery of a role for the pancreas in diabetes is generally ascribed to Joseph von Mering
and Oskar Minkowski
, who in 1889 found that dogs whose pancreas was removed developed all the signs and symptoms of diabetes and died shortly afterwards.
In 1910, Sir Edward Albert Sharpey-Schafer suggested that people with diabetes were deficient in a single chemical that was normally produced by the pancreas—he proposed calling this substance insulin, from the Latin insula, meaning island, in reference to the insulin-producing islets of Langerhans
in the pancreas.
The endocrine role of the pancreas in metabolism, and indeed the existence of insulin, was not further clarified until 1921, when Sir Frederick Grant Banting and Charles Herbert Best repeated the work of Von Mering and Minkowski, and went further to demonstrate they could reverse induced diabetes in dogs by giving them an extract from the pancreatic islets of Langerhans of healthy dogs.
Banting, Best, and colleagues (especially the chemist Collip
) went on to purify the hormone insulin from bovine pancreases at the University of Toronto
. This led to the availability of an effective treatment—insulin injections—and the first patient was treated in 1922. For this, Banting and laboratory director MacLeod received the Nobel Prize in Physiology or Medicine
in 1923; both shared their Prize money with others in the team who were not recognized, in particular Best and Collip. Banting and Best made the patent available without charge and did not attempt to control commercial production. Insulin
production and therapy rapidly spread around the world, largely as a result of this decision. Banting is honored by World Diabetes Day
which is held on his birthday, November 14.
The distinction between what is now known as type 1 diabetes and type 2 diabetes was first clearly made by Sir Harold Percival (Harry) Himsworth
, and published in January 1936.
Despite the availability of treatment, diabetes has remained a major cause of death. For instance, statistics
reveal that the cause-specific mortality rate
during 1927 amounted to about 47.7 per 100,000 population in Malta
.
Other landmark discoveries include:
In 1980, U.S. biotech company Genentech developed biosynthetic human insulin. The insulin was isolated from genetically altered bacteria (the bacteria contain the human gene for synthesizing synthetic human insulin), which produce large quantities of insulin. The purified insulin is distributed to pharmacies for use by diabetes patients. Initially, this development was not regarded by the medical profession as a clinically meaningful development. However, by 1996, the advent of insulin analogues which had vastly improved absorption, distribution, metabolism, and excretion (ADME)
characteristics which were clinically meaningful based on this early biotechnology development.
" was the result of international efforts to improve the care accorded to those with diabetes. Doing so is important both in terms of quality of life and life expectancy but also economically—expenses due to diabetes have been shown to be a major drain on health-and productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve treatment of the disease.
A study shows that diabetic patients with neuropathic symptoms such as numbness
or tingling in feet or hands are twice as likely to be unemployed as those without the symptoms.
. The symptoms may relate to fluid loss and polyuria, but the course may also be insidious. Diabetic animals are more prone to infections. The long-term complications recognised in humans are much rarer in animals. The principles of treatment (weight loss, oral antidiabetics, subcutaneous insulin) and management of emergencies (e.g. ketoacidosis) are similar to those in humans.
Blood sugar
The blood sugar concentration or blood glucose level is the amount of glucose present in the blood of a human or animal. Normally in mammals, the body maintains the blood glucose level at a reference range between about 3.6 and 5.8 mM , or 64.8 and 104.4 mg/dL...
, either because the body does not produce enough insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
, or because cells do not respond to the insulin that is produced. This high blood sugar produces the classical symptoms of polyuria
Polyuria
Polyuria is a condition usually defined as excessive or abnormally large production or passage of urine . Frequent urination is sometimes included by definition, but is nonetheless usually an accompanying symptom...
(frequent urination), polydipsia
Polydipsia
Polydipsia is a medical symptom in which the patient displays excessive thirst. The word derives from the Greek πολυδιψία, which is derived from πολύς + δίψα...
(increased thirst) and polyphagia
Polyphagia
Polyphagia means "eating too much". It derives from the Greek words πολύς which means "very much", and φαγῶ , verb for "I eat"....
(increased hunger).
There are three main types of diabetes:
- Type 1 diabetesDiabetes mellitus type 1Diabetes mellitus type 1 is a form of diabetes mellitus that results from autoimmune destruction of insulin-producing beta cells of the pancreas. The subsequent lack of insulin leads to increased blood and urine glucose...
: results from the body's failure to produce insulin, and presently requires the person to inject insulin. (Also referred to as insulin-dependent diabetes mellitus, IDDM for short, and juvenile diabetes.) - Type 2 diabetesDiabetes mellitus type 2Diabetes mellitus type 2formerly non-insulin-dependent diabetes mellitus or adult-onset diabetesis a metabolic disorder that is characterized by high blood glucose in the context of insulin resistance and relative insulin deficiency. Diabetes is often initially managed by increasing exercise and...
: results from insulin resistanceInsulin resistanceInsulin resistance is a physiological condition where the natural hormone insulin becomes less effective at lowering blood sugars. The resulting increase in blood glucose may raise levels outside the normal range and cause adverse health effects, depending on dietary conditions. Certain cell types...
, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. (Formerly referred to as non-insulin-dependent diabetes mellitus, NIDDM for short, and adult-onset diabetes.) - Gestational diabetesGestational diabetesGestational diabetes is a condition in which women without previously diagnosed diabetes exhibit high blood glucose levels during pregnancy . It is widely accepted as a disease only in the United States, there is some question whether the condition is natural during pregnancy...
: is when pregnant women, who have never had diabetes before, have a high blood glucose level during pregnancy. It may precede development of type 2 DM.
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes
Mody
Mody may refer to:* Maturity onset diabetes of the young * Hormusjee Naorojee Mody...
.
All forms of diabetes have been treatable since insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
became available in 1921, and type 2 diabetes may be controlled with medications. Both type 1 and 2 are chronic
Chronic (medicine)
A chronic disease is a disease or other human health condition that is persistent or long-lasting in nature. The term chronic is usually applied when the course of the disease lasts for more than three months. Common chronic diseases include asthma, cancer, diabetes and HIV/AIDS.In medicine, the...
conditions that usually cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery
Gastric bypass surgery
Gastric bypass procedures are any of a group of similar operations that first divides the stomach into a small upper pouch and a much larger lower "remnant" pouch and then re-arranges the small intestine to allow both pouches to stay connected to it. Surgeons have developed several different ways...
has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycemia
Hypoglycemia
Hypoglycemia or hypoglycæmia is the medical term for a state produced by a lower than normal level of blood glucose. The term literally means "under-sweet blood"...
, diabetic ketoacidosis
Diabetic ketoacidosis
Diabetic ketoacidosis is a potentially life-threatening complication in patients with diabetes mellitus. It happens predominantly in those with type 1 diabetes, but it can occur in those with type 2 diabetes under certain circumstances...
, or nonketotic hyperosmolar coma
Nonketotic hyperosmolar coma
Nonketotic hyperosmolar coma is a type of diabetic coma associated with a high mortality seen in diabetes mellitus type 2. The preferred term used by the American Diabetes Association is hyperosmolar nonketotic state . Other commonly used names are hyperosmolar hyperglycemic nonketotic coma or...
. Serious long-term complications include cardiovascular disease
Cardiovascular disease
Heart disease or cardiovascular disease are the class of diseases that involve the heart or blood vessels . While the term technically refers to any disease that affects the cardiovascular system , it is usually used to refer to those related to atherosclerosis...
, chronic renal failure
Chronic renal failure
Chronic kidney disease , also known as chronic renal disease, is a progressive loss in renal function over a period of months or years. The symptoms of worsening kidney function are unspecific, and might include feeling generally unwell and experiencing a reduced appetite...
, retinal damage
Diabetic retinopathy
Diabetic retinopathy is retinopathy caused by complications of diabetes mellitus, which can eventually lead to blindness....
. Adequate treatment of diabetes is thus important, as well as blood pressure
Blood pressure
Blood pressure is the pressure exerted by circulating blood upon the walls of blood vessels, and is one of the principal vital signs. When used without further specification, "blood pressure" usually refers to the arterial pressure of the systemic circulation. During each heartbeat, BP varies...
control and lifestyle factors such as smoking
Tobacco smoking
Tobacco smoking is the practice where tobacco is burned and the resulting smoke is inhaled. The practice may have begun as early as 5000–3000 BCE. Tobacco was introduced to Eurasia in the late 16th century where it followed common trade routes...
cessation and maintaining a healthy body weight.
As of 2000 at least 171 million people worldwide have diabetes, or 2.8% of the population. Type 2 diabetes is by far the most common, affecting 90 to 95% of the U.S. diabetes population.
Classification
Most cases of diabetes mellitus fall into three broad categories: type 1Diabetes mellitus type 1
Diabetes mellitus type 1 is a form of diabetes mellitus that results from autoimmune destruction of insulin-producing beta cells of the pancreas. The subsequent lack of insulin leads to increased blood and urine glucose...
, type 2
Diabetes mellitus type 2
Diabetes mellitus type 2formerly non-insulin-dependent diabetes mellitus or adult-onset diabetesis a metabolic disorder that is characterized by high blood glucose in the context of insulin resistance and relative insulin deficiency. Diabetes is often initially managed by increasing exercise and...
, and gestational diabetes
Gestational diabetes
Gestational diabetes is a condition in which women without previously diagnosed diabetes exhibit high blood glucose levels during pregnancy . It is widely accepted as a disease only in the United States, there is some question whether the condition is natural during pregnancy...
. A few other types are described. The term diabetes, without qualification, usually refers to diabetes mellitus. The rare disease diabetes insipidus
Diabetes insipidus
Diabetes insipidus is a condition characterized by excessive thirst and excretion of large amounts of severely diluted urine, with reduction of fluid intake having no effect on the concentration of the urine. There are several different types of DI, each with a different cause...
has similar symptoms as diabetes mellitus, but without disturbances in the sugar metabolism (insipidus meaning "without taste" in Latin).
| Comparison of type 1 and 2 diabetes | ||
|---|---|---|
| Feature | Type 1 diabetes | Type 2 diabetes |
| Onset | Sudden | Gradual |
| Age at onset | Any age (mostly young) |
Mostly in adults |
| Body habitus | Thin or normal | Often obese |
| Ketoacidosis Diabetic ketoacidosis Diabetic ketoacidosis is a potentially life-threatening complication in patients with diabetes mellitus. It happens predominantly in those with type 1 diabetes, but it can occur in those with type 2 diabetes under certain circumstances... |
Common | Rare |
| Autoantibodies | Usually present | Absent |
| Endogenous insulin | Low or absent | Normal, decreased or increased |
| Concordance Concordance (genetics) Concordance as used in genetics usually means the presence of the same trait in both members of a pair of twins. However, the strict definition is the probability that a pair of individuals will both have a certain characteristic, given that one of the pair has the characteristic. For example,... in identical twins |
50% | 90% |
| Prevalence | Less prevalent | More prevalent - 90 to 95% of U.S. diabetics |
The term "type 1 diabetes" has replaced several former terms, including childhood-onset diabetes, juvenile diabetes, and insulin-dependent diabetes mellitus (IDDM). Likewise, the term "type 2 diabetes" has replaced several former terms, including adult-onset diabetes, obesity-related diabetes, and non-insulin-dependent diabetes mellitus (NIDDM). Beyond these two types, there is no agreed-upon standard nomenclature. Various sources have defined "type 3 diabetes" as: gestational diabetes
Gestational diabetes
Gestational diabetes is a condition in which women without previously diagnosed diabetes exhibit high blood glucose levels during pregnancy . It is widely accepted as a disease only in the United States, there is some question whether the condition is natural during pregnancy...
, insulin-resistant type 1 diabetes (or "double diabetes"), type 2 diabetes which has progressed to require injected insulin, and latent autoimmune diabetes
Latent autoimmune diabetes
Latent Autoimmune Diabetes of Adults , also known as, Diabetes Type 1.5, is a term coined by Tuomi et al. in 1993 to describe slow-onset Type 1 autoimmune diabetes in adults...
of adults (or LADA or "type 1.5
Diabetes type 1.5
Diabetes type 1.5 is a term applied to:* Latent autoimmune diabetes in adults* Ketosis-prone diabetes mellitus type 2...
" diabetes).
Type 1 diabetes
Type 1 diabetes mellitus is characterized by loss of the insulin-producing beta cellBeta cell
Beta cells are a type of cell in the pancreas located in the so-called islets of Langerhans. They make up 65-80% of the cells in the islets.-Function:...
s of the islets of Langerhans
Islets of Langerhans
The islets of Langerhans are the regions of the pancreas that contain its endocrine cells. Discovered in 1869 by German pathological anatomist Paul Langerhans at the age of 22, the islets of Langerhans constitute approximately 1 to 2% of the mass of the pancreas...
in the pancreas leading to insulin deficiency. This type of diabetes can be further classified as immune-mediated or idiopathic. The majority of type 1 diabetes is of the immune-mediated nature, where beta cell loss is a T-cell mediated autoimmune
Autoimmunity
Autoimmunity is the failure of an organism to recognize its own constituent parts as self, which allows an immune response against its own cells and tissues. Any disease that results from such an aberrant immune response is termed an autoimmune disease...
attack. There is no known preventive measure against type 1 diabetes, which causes approximately 10% of diabetes mellitus cases in North America and Europe. Most affected people are otherwise healthy and of a healthy weight when onset occurs. Sensitivity and responsiveness to insulin are usually normal, especially in the early stages. Type 1 diabetes can affect children or adults but was traditionally termed "juvenile diabetes" because it represents a majority of the diabetes cases in children.
"Brittle" diabetes, also known as unstable diabetes or labile diabetes, is a term that was traditionally used to describe to dramatic and recurrent swings in glucose
Glucose
Glucose is a simple sugar and an important carbohydrate in biology. Cells use it as the primary source of energy and a metabolic intermediate...
levels, often occurring for no apparent reason in insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
-dependent diabetes. This term, however, has no biologic basis and should not be used. There are many different reasons for type 1 diabetes to be accompanied by irregular and unpredictable hyperglycemia
Hyperglycemia
Hyperglycemia or Hyperglycæmia, or high blood sugar, is a condition in which an excessive amount of glucose circulates in the blood plasma. This is generally a glucose level higher than 13.5mmol/l , but symptoms may not start to become noticeable until even higher values such as 15-20 mmol/l...
s, frequently with ketosis
Ketosis
Ketosis is a state of elevated levels of ketone bodies in the body. It is almost always generalized throughout the body, with hyperketonemia, that is, an elevated level of ketone bodies in the blood. Ketone bodies are formed by ketogenesis when the liver glycogen stores are depleted...
, and sometimes serious hypoglycemia
Hypoglycemia
Hypoglycemia or hypoglycæmia is the medical term for a state produced by a lower than normal level of blood glucose. The term literally means "under-sweet blood"...
s, including an impaired counterregulatory response to hypoglycemia, occult infection, gastroparesis (which leads to erratic absorption of dietary carbohydrates), and endocrinopathies (eg, Addison's disease). These phenomena are believed to occur no more frequently than in 1% to 2% of persons with type 1 diabetes.
Type 2 diabetes
Type 2 diabetes mellitus is characterized by insulin resistanceInsulin resistance
Insulin resistance is a physiological condition where the natural hormone insulin becomes less effective at lowering blood sugars. The resulting increase in blood glucose may raise levels outside the normal range and cause adverse health effects, depending on dietary conditions. Certain cell types...
which may be combined with relatively reduced insulin secretion. The defective responsiveness of body tissues to insulin is believed to involve the insulin receptor
Insulin receptor
In molecular biology, the insulin receptor is a transmembrane receptor that is activated by insulin. It belongs to the large class of tyrosine kinase receptors....
. However, the specific defects are not known. Diabetes mellitus due to a known defect are classified separately. Type 2 diabetes is the most common type.
In the early stage of type 2 diabetes, the predominant abnormality is reduced insulin sensitivity. At this stage hyperglycemia can be reversed by a variety of measures and medications
Anti-diabetic drug
Anti-diabetic medications treat diabetes mellitus by lowering glucose levels in the blood. With the exceptions of insulin, exenatide, and pramlintide, all are administered orally and are thus also called oral hypoglycemic agents or oral antihyperglycemic agents...
that improve insulin sensitivity or reduce glucose production by the liver
Liver
The liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion...
.
Gestational diabetes
Gestational diabetes mellitus (GDM) resembles type 2 diabetes in several respects, involving a combination of relatively inadequate insulin secretion and responsiveness. It occurs in about 2%–5% of all pregnanciesPregnancy
Pregnancy refers to the fertilization and development of one or more offspring, known as a fetus or embryo, in a woman's uterus. In a pregnancy, there can be multiple gestations, as in the case of twins or triplets...
and may improve or disappear after delivery. Gestational diabetes is fully treatable but requires careful medical supervision throughout the pregnancy. About 20%–50% of affected women develop type 2 diabetes later in life.
Even though it may be transient, untreated gestational diabetes can damage the health of the fetus or mother. Risks to the baby include macrosomia (high birth weight), congenital cardiac and central nervous system anomalies, and skeletal muscle malformations. Increased fetal insulin may inhibit fetal surfactant
Surfactant
Surfactants are compounds that lower the surface tension of a liquid, the interfacial tension between two liquids, or that between a liquid and a solid...
production and cause respiratory distress syndrome
Infant respiratory distress syndrome
Infant respiratory distress syndrome , also called neonatal respiratory distress syndrome or respiratory distress syndrome of newborn, previously called hyaline membrane disease, is a syndrome in premature infants caused by developmental insufficiency of surfactant production and structural...
. Hyperbilirubinemia may result from red blood cell destruction. In severe cases, perinatal death may occur, most commonly as a result of poor placental perfusion due to vascular impairment. Labor induction may be indicated with decreased placental function. A cesarean section
Caesarean section
A Caesarean section, is a surgical procedure in which one or more incisions are made through a mother's abdomen and uterus to deliver one or more babies, or, rarely, to remove a dead fetus...
may be performed if there is marked fetal distress or an increased risk of injury associated with macrosomia, such as shoulder dystocia
Shoulder dystocia
Shoulder dystocia is a specific case of dystocia whereby after the delivery of the head, the anterior shoulder of the infant cannot pass below the pubic symphysis, or requires significant manipulation to pass below the pubic symphysis. It is diagnosed when the shoulders fail to deliver shortly...
.
A 2008 study completed in the U.S. found that the number of American women entering pregnancy with preexisting diabetes is increasing. In fact the rate of diabetes in expectant mothers has more than doubled in the past 6 years. This is particularly problematic as diabetes raises the risk of complications during pregnancy, as well as increasing the potential that the children of diabetic mothers will also become diabetic in the future.
Other types
Pre-diabetes indicates a condition that occurs when a person's blood glucose levels are higher than normal but not high enough for a diagnosis of type 2 diabetes.Many people destined to develop type 2 diabetes spend many years in a state of pre-diabetes which has been termed "America's largest healthcare epidemic."
Latent autoimmune diabetes of adults is a condition in which Type 1 diabetes develops in adults. Adults with LADA are frequently initially misdiagnosed as having Type 2 diabetes, based on age rather than etiology
Etiology
Etiology is the study of causation, or origination. The word is derived from the Greek , aitiologia, "giving a reason for" ....
.
Some cases of diabetes are caused by the body's tissue receptors not responding to insulin (even when insulin levels are normal, which is what separates it from type 2 diabetes); this form is very uncommon. Genetic mutations (autosomal or mitochondrial) can lead to defects in beta cell
Beta cell
Beta cells are a type of cell in the pancreas located in the so-called islets of Langerhans. They make up 65-80% of the cells in the islets.-Function:...
function. Abnormal insulin action may also have been genetically determined in some cases. Any disease that causes extensive damage to the pancreas
Pancreas
The pancreas is a gland organ in the digestive and endocrine system of vertebrates. It is both an endocrine gland producing several important hormones, including insulin, glucagon, and somatostatin, as well as a digestive organ, secreting pancreatic juice containing digestive enzymes that assist...
may lead to diabetes (for example, chronic pancreatitis
Chronic pancreatitis
Chronic pancreatitis is a long-standing inflammation of the pancreas that alters its normal structure and functions. It can present as episodes of acute inflammation in a previously injured pancreas, or as chronic damage with persistent pain or malabsorption....
and cystic fibrosis
Cystic fibrosis
Cystic fibrosis is a recessive genetic disease affecting most critically the lungs, and also the pancreas, liver, and intestine...
). Diseases associated with excessive secretion of insulin-antagonistic
Insulin receptor
In molecular biology, the insulin receptor is a transmembrane receptor that is activated by insulin. It belongs to the large class of tyrosine kinase receptors....
hormone
Hormone
A hormone is a chemical released by a cell or a gland in one part of the body that sends out messages that affect cells in other parts of the organism. Only a small amount of hormone is required to alter cell metabolism. In essence, it is a chemical messenger that transports a signal from one...
s can cause diabetes (which is typically resolved once the hormone excess is removed). Many drugs impair insulin secretion and some toxins damage pancreatic beta cells. The ICD
ICD
The International Statistical Classification of Diseases and Related Health Problems is a medical classification that provides codes to classify diseases and a wide variety of signs, symptoms, abnormal findings, complaints, social circumstances, and external causes of injury or disease...
-10 (1992) diagnostic entity, malnutrition-related diabetes mellitus (MRDM or MMDM, ICD-10 code E12), was deprecated by the World Health Organization
World Health Organization
The World Health Organization is a specialized agency of the United Nations that acts as a coordinating authority on international public health. Established on 7 April 1948, with headquarters in Geneva, Switzerland, the agency inherited the mandate and resources of its predecessor, the Health...
when the current taxonomy was introduced in 1999.
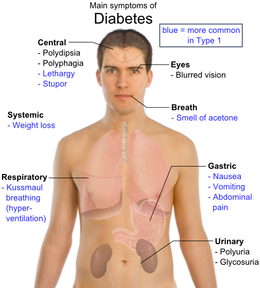
Signs and symptoms
Hyperglycemia and osmosis
The classical symptoms of diabetes are polyuriaPolyuria
Polyuria is a condition usually defined as excessive or abnormally large production or passage of urine . Frequent urination is sometimes included by definition, but is nonetheless usually an accompanying symptom...
(frequent urination), polydipsia
Polydipsia
Polydipsia is a medical symptom in which the patient displays excessive thirst. The word derives from the Greek πολυδιψία, which is derived from πολύς + δίψα...
(increased thirst) and polyphagia
Polyphagia
Polyphagia means "eating too much". It derives from the Greek words πολύς which means "very much", and φαγῶ , verb for "I eat"....
(increased hunger). Symptoms may develop rapidly (weeks or months) in type 1 diabetes while in type 2 diabetes they usually develop much more slowly and may be subtle or absent.
Prolonged high blood glucose causes glucose absorption, which leads to changes in the shape of the lenses of the eyes, resulting in vision changes; sustained sensible glucose control usually returns the lens to its original shape. Blurred vision is a common complaint leading to a diabetes diagnosis; type 1 should always be suspected in cases of rapid vision change, whereas with type 2 change is generally more gradual, but should still be suspected .
Diabetic emergencies
People (usually with type 1 diabetes) may also present with diabetic ketoacidosisDiabetic ketoacidosis
Diabetic ketoacidosis is a potentially life-threatening complication in patients with diabetes mellitus. It happens predominantly in those with type 1 diabetes, but it can occur in those with type 2 diabetes under certain circumstances...
, a state of metabolic dysregulation characterized by the smell of acetone
Acetone
Acetone is the organic compound with the formula 2CO, a colorless, mobile, flammable liquid, the simplest example of the ketones.Acetone is miscible with water and serves as an important solvent in its own right, typically as the solvent of choice for cleaning purposes in the laboratory...
; a rapid, deep breathing known as Kussmaul breathing
Kussmaul breathing
Kussmaul breathing is a deep and labored breathing pattern often associated with severe metabolic acidosis, particularly diabetic ketoacidosis but also renal failure. It is a form of hyperventilation, which is any breathing pattern that reduces carbon dioxide in the blood due to increased rate or...
; nausea; vomiting and abdominal pain
Abdominal pain
Abdominal pain can be one of the symptoms associated with transient disorders or serious disease. Making a definitive diagnosis of the cause of abdominal pain can be difficult, because many diseases can result in this symptom. Abdominal pain is a common problem...
; and altered states of consciousness.
A rarer but equally severe possibility is hyperosmolar nonketotic state
Nonketotic hyperosmolar coma
Nonketotic hyperosmolar coma is a type of diabetic coma associated with a high mortality seen in diabetes mellitus type 2. The preferred term used by the American Diabetes Association is hyperosmolar nonketotic state . Other commonly used names are hyperosmolar hyperglycemic nonketotic coma or...
, which is more common in type 2 diabetes and is mainly the result of dehydration. Often, the patient has been drinking extreme amounts of sugar-containing drinks, leading to a vicious circle
Positive feedback
Positive feedback is a process in which the effects of a small disturbance on a system include an increase in the magnitude of the perturbation. That is, A produces more of B which in turn produces more of A. In contrast, a system that responds to a perturbation in a way that reduces its effect is...
in regard to the water loss.
Complications
All forms of diabetes increase the risk of long-term complications. These typically develop after many years (10–20), but may be the first symptom in those who have otherwise not received a diagnosis before that time. The major long-term complications relate to damage to blood vesselBlood vessel
The blood vessels are the part of the circulatory system that transports blood throughout the body. There are three major types of blood vessels: the arteries, which carry the blood away from the heart; the capillaries, which enable the actual exchange of water and chemicals between the blood and...
s.
Diabetes doubles the risk of cardiovascular disease
Cardiovascular disease
Heart disease or cardiovascular disease are the class of diseases that involve the heart or blood vessels . While the term technically refers to any disease that affects the cardiovascular system , it is usually used to refer to those related to atherosclerosis...
. The main "macrovascular" diseases
Macrovascular disease
Macrovascular disease is a disease of any large blood vessels in the body. It is a disease of the large blood vessels, including the coronary arteries, the aorta, and the sizable arteries in the brain and in the limbs....
(related to atherosclerosis
Atherosclerosis
Atherosclerosis is a condition in which an artery wall thickens as a result of the accumulation of fatty materials such as cholesterol...
of larger arteries) are ischemic heart disease (angina
Angina
Angina pectoris, commonly known as angina, is chest pain due to ischemia of the heart muscle, generally due to obstruction or spasm of the coronary arteries . Coronary artery disease, the main cause of angina, is due to atherosclerosis of the cardiac arteries...
and myocardial infarction
Myocardial infarction
Myocardial infarction or acute myocardial infarction , commonly known as a heart attack, results from the interruption of blood supply to a part of the heart, causing heart cells to die...
), stroke
Stroke
A stroke, previously known medically as a cerebrovascular accident , is the rapidly developing loss of brain function due to disturbance in the blood supply to the brain. This can be due to ischemia caused by blockage , or a hemorrhage...
and peripheral vascular disease.
Diabetes also causes "microvascular" complications—damage to the small blood vessels. Diabetic retinopathy
Diabetic retinopathy
Diabetic retinopathy is retinopathy caused by complications of diabetes mellitus, which can eventually lead to blindness....
, which affects blood vessel formation in the retina
Retina
The vertebrate retina is a light-sensitive tissue lining the inner surface of the eye. The optics of the eye create an image of the visual world on the retina, which serves much the same function as the film in a camera. Light striking the retina initiates a cascade of chemical and electrical...
of the eye, can lead to visual symptoms, reduced vision, and potentially blindness
Blindness
Blindness is the condition of lacking visual perception due to physiological or neurological factors.Various scales have been developed to describe the extent of vision loss and define blindness...
. Diabetic nephropathy
Diabetic nephropathy
Diabetic nephropathy , also known as Kimmelstiel-Wilson syndrome, or nodular diabetic glomerulosclerosis and intercapillary glomerulonephritis, is a progressive kidney disease caused by angiopathy of capillaries in the kidney glomeruli. It is characterized by nephrotic syndrome and diffuse...
, the impact of diabetes on the kidneys, can lead to scarring changes in the kidney tissue
Glomerulosclerosis
Glomerulosclerosis refers to a hardening of the glomerulus in the kidney. It is a general term to describe scarring of the kidneys' tiny blood vessels, the glomeruli, the functional units in the kidney that filter urine from the blood....
, loss of small
Microalbuminuria
Microalbuminuria occurs when the kidney leaks small amounts of albumin into the urine, in other words, when there is an abnormally high permeability for albumin in the renal glomerulus.-Diagnosis:...
or progressively larger
Proteinuria
Proteinuria means the presence of anexcess of serum proteins in the urine. The protein in the urine often causes the urine to become foamy, although foamy urine may also be caused by bilirubin in the urine , retrograde ejaculation, pneumaturia due to a fistula, or drugs such as pyridium.- Causes...
amounts of protein in the urine, and eventually chronic kidney disease requiring dialysis
Dialysis
In medicine, dialysis is a process for removing waste and excess water from the blood, and is primarily used to provide an artificial replacement for lost kidney function in people with renal failure...
. Diabetic neuropathy
Diabetic neuropathy
Diabetic neuropathies are neuropathic disorders that are associated with diabetes mellitus. These conditions are thought to result from diabetic microvascular injury involving small blood vessels that supply nerves in addition to macrovascular conditions that can culminate in diabetic neuropathy...
is the impact of diabetes on the nervous system
Peripheral nervous system
The peripheral nervous system consists of the nerves and ganglia outside of the brain and spinal cord. The main function of the PNS is to connect the central nervous system to the limbs and organs. Unlike the CNS, the PNS is not protected by the bone of spine and skull, or by the blood–brain...
, most commonly causing numbness, tingling and pain in the feet and also increasing the risk of skin damage due to altered sensation. Together with vascular disease in the legs, neuropathy contributes to the risk of diabetes-related foot problems
Diabetic foot
Diabetic foot ulcer is one of the major complications of diabetes mellitus, and probably the major component of the diabetic foot. It occurs in 15% of all patients with diabetes and precedes 84% of all lower leg amputations...
(such as diabetic foot ulcers) that can be difficult to treat and occasionally require amputation
Amputation
Amputation is the removal of a body extremity by trauma, prolonged constriction, or surgery. As a surgical measure, it is used to control pain or a disease process in the affected limb, such as malignancy or gangrene. In some cases, it is carried out on individuals as a preventative surgery for...
.
Other problems
A number of skin rashes can occur in diabetes that are collectively known as diabetic dermadromes.Causes
The cause of diabetes depends on the type.Type 1 diabetes is partly inherited and then triggered by certain infections, with some evidence pointing at Coxsackie B4 virus
Coxsackie B4 virus
Coxsackie B4 virus is a virus which can trigger an autoimmune reaction which results in destruction of the insulin-producing beta cells of the pancreas, which is one of several different etiologies of diabetes mellitus....
. There is a genetic element in individual susceptibility to some of these triggers which has been traced to particular HLA
Human leukocyte antigen
The human leukocyte antigen system is the name of the major histocompatibility complex in humans. The super locus contains a large number of genes related to immune system function in humans. This group of genes resides on chromosome 6, and encodes cell-surface antigen-presenting proteins and...
genotype
Genotype
The genotype is the genetic makeup of a cell, an organism, or an individual usually with reference to a specific character under consideration...
s (i.e., the genetic "self" identifiers relied upon by the immune system). However, even in those who have inherited the susceptibility, type 1 diabetes mellitus seems to require an environmental trigger.
Type 2 diabetes is due primarily to lifestyle factors and genetics.
Following is a comprehensive list of other causes of diabetes:
- Genetic defects of β-cell Function
- Maturity onset diabetes of the youngMaturity onset diabetes of the youngMaturity onset diabetes of the young refers to any of several hereditary forms of diabetes caused by mutations in an autosomal dominant gene disrupting insulin production...
(MODY) - Mitochondrial DNA mutations
- Maturity onset diabetes of the young
- Genetic defects in insulin processing or insulin action
- Defects in proinsulinProinsulinProinsulin is the prohormone precursor to insulin made in the beta cells of the islets of Langerhans, specialized regions of the pancreas. In humans, proinsulin is encoded by the INS gene.- Synthesis and post-translational modification :...
conversion - Insulin gene mutations
- Insulin receptor mutations
- Defects in proinsulin
- Exocrine Pancreatic Defects
- Chronic pancreatitisChronic pancreatitisChronic pancreatitis is a long-standing inflammation of the pancreas that alters its normal structure and functions. It can present as episodes of acute inflammation in a previously injured pancreas, or as chronic damage with persistent pain or malabsorption....
- PancreatectomyPancreatectomyIn medicine, a pancreatectomy is the surgical removal of all or part of the pancreas. Several types of pancreatectomy exist, including pancreaticoduodenectomy , distal pancreatectomy, segmental pancreatectomy, and total pancreatectomy...
- Pancreatic neoplasia
- Cystic fibrosisCystic fibrosisCystic fibrosis is a recessive genetic disease affecting most critically the lungs, and also the pancreas, liver, and intestine...
- Hemochromatosis
- Fibrocalculous pancreatopathy
- Chronic pancreatitis
- Endocrinopathies
- Growth hormone excess (acromegalyAcromegalyAcromegaly is a syndrome that results when the anterior pituitary gland produces excess growth hormone after epiphyseal plate closure at puberty...
) - Cushing syndrome
- HyperthyroidismHyperthyroidismHyperthyroidism is the term for overactive tissue within the thyroid gland causing an overproduction of thyroid hormones . Hyperthyroidism is thus a cause of thyrotoxicosis, the clinical condition of increased thyroid hormones in the blood. Hyperthyroidism and thyrotoxicosis are not synonymous...
- PheochromocytomaPheochromocytomaA pheochromocytoma or phaeochromocytoma is a neuroendocrine tumor of the medulla of the adrenal glands , or extra-adrenal chromaffin tissue that failed to involute after birth and secretes excessive amounts of catecholamines, usually noradrenaline , and adrenaline to a lesser extent...
- GlucagonomaGlucagonomaA glucagonoma is a rare tumor of the alpha cells of the pancreas that results in up to a 1000-fold overproduction of the hormone glucagon. Alpha cell tumors are commonly associated with glucagonoma syndrome, though similar symptoms are present in cases of pseudoglucagonoma syndrome in the absence...
- Growth hormone excess (acromegaly
- Infections
- Cytomegalovirus infection
- Coxsackievirus BCoxsackie B4 virusCoxsackie B4 virus is a virus which can trigger an autoimmune reaction which results in destruction of the insulin-producing beta cells of the pancreas, which is one of several different etiologies of diabetes mellitus....
- Drugs
- Glucocorticoids
- Thyroid hormoneThyroid hormoneThe thyroid hormones, thyroxine and triiodothyronine , are tyrosine-based hormones produced by the thyroid gland primarily responsible for regulation of metabolism. An important component in the synthesis of thyroid hormones is iodine. The major form of thyroid hormone in the blood is thyroxine ,...
- β-adrenergic agonists
Pathophysiology
Glucose
Glucose is a simple sugar and an important carbohydrate in biology. Cells use it as the primary source of energy and a metabolic intermediate...
from the blood into most cells (primarily muscle and fat cells, but not central nervous system cells). Therefore deficiency of insulin or the insensitivity of its receptors
Receptor (biochemistry)
In biochemistry, a receptor is a molecule found on the surface of a cell, which receives specific chemical signals from neighbouring cells or the wider environment within an organism...
plays a central role in all forms of diabetes mellitus.
Humans are capable of digesting some carbohydrates
Carbohydrate metabolism
Carbohydrate metabolism denotes the various biochemical processes responsible for the formation, breakdown and interconversion of carbohydrates in living organisms....
, in particular those most common in food; starch, and some disaccharides such as sucrose, are converted within a few hours to simpler forms most notably the monosaccharide
Monosaccharide
Monosaccharides are the most basic units of biologically important carbohydrates. They are the simplest form of sugar and are usually colorless, water-soluble, crystalline solids. Some monosaccharides have a sweet taste. Examples of monosaccharides include glucose , fructose , galactose, xylose...
glucose
Glucose
Glucose is a simple sugar and an important carbohydrate in biology. Cells use it as the primary source of energy and a metabolic intermediate...
, the principal carbohydrate energy source used by the body. The rest are passed on for processing by gut flora largely in the colon. Insulin is released into the blood by beta cells (β-cells), found in the Islets of Langerhans in the pancreas, in response to rising levels of blood glucose, typically after eating. Insulin is used by about two-thirds of the body's cells to absorb glucose from the blood for use as fuel, for conversion to other needed molecules, or for storage.
Insulin is also the principal control signal for conversion of glucose to glycogen
Glycogen
Glycogen is a molecule that serves as the secondary long-term energy storage in animal and fungal cells, with the primary energy stores being held in adipose tissue...
for internal storage in liver and muscle cells. Lowered glucose levels result both in the reduced release of insulin from the beta cells and in the reverse conversion of glycogen to glucose when glucose levels fall. This is mainly controlled by the hormone glucagon
Glucagon
Glucagon, a hormone secreted by the pancreas, raises blood glucose levels. Its effect is opposite that of insulin, which lowers blood glucose levels. The pancreas releases glucagon when blood sugar levels fall too low. Glucagon causes the liver to convert stored glycogen into glucose, which is...
which acts in the opposite manner to insulin. Glucose thus forcibly produced from internal liver cell stores (as glycogen) re-enters the bloodstream; muscle cells lack the necessary export mechanism. Normally liver cells do this when the level of insulin is low (which normally correlates with low levels of blood glucose).
Higher insulin levels increase some anabolic
Anabolism
Anabolism is the set of metabolic pathways that construct molecules from smaller units. These reactions require energy. One way of categorizing metabolic processes, whether at the cellular, organ or organism level is as 'anabolic' or as 'catabolic', which is the opposite...
("building up") processes such as cell growth and duplication, protein synthesis
Protein biosynthesis
Protein biosynthesis is the process in which cells build or manufacture proteins. The term is sometimes used to refer only to protein translation but more often it refers to a multi-step process, beginning with amino acid synthesis and transcription of nuclear DNA into messenger RNA, which is then...
, and fat
Lipid
Lipids constitute a broad group of naturally occurring molecules that include fats, waxes, sterols, fat-soluble vitamins , monoglycerides, diglycerides, triglycerides, phospholipids, and others...
storage. Insulin (or its lack) is the principal signal in converting many of the bidirectional processes of metabolism from a catabolic
Catabolism
Catabolism is the set of metabolic pathways that break down molecules into smaller units and release energy. In catabolism, large molecules such as polysaccharides, lipids, nucleic acids and proteins are broken down into smaller units such as monosaccharides, fatty acids, nucleotides, and amino...
to an anabolic direction, and vice versa. In particular, a low insulin level is the trigger for entering or leaving ketosis (the fat burning metabolic phase).
If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or resistance
Insulin resistance
Insulin resistance is a physiological condition where the natural hormone insulin becomes less effective at lowering blood sugars. The resulting increase in blood glucose may raise levels outside the normal range and cause adverse health effects, depending on dietary conditions. Certain cell types...
), or if the insulin itself is defective, then glucose will not have its usual effect so that glucose will not be absorbed properly by those body cells that require it nor will it be stored appropriately in the liver and muscles. The net effect is persistent high levels of blood glucose, poor protein synthesis, and other metabolic derangements, such as acidosis
Acidosis
Acidosis is an increased acidity in the blood and other body tissue . If not further qualified, it usually refers to acidity of the blood plasma....
.
When the glucose concentration in the blood is raised beyond its renal threshold
Renal threshold
In physiology, the renal threshold is the concentration of a substance dissolved in the blood above which the kidneys begin to remove it into the urine. When the renal threshold of a substance is exceeded, reabsorption of the substance by the proximal renal tubuli is incomplete; consequently, part...
(about 10 mmol/L, although this may be altered in certain conditions, such as pregnancy), reabsorption
Reabsorption
In physiology, reabsorption or tubular reabsorption is the flow of glomerular filtrate from the proximal tubule of the nephron into the peritubular capillaries, or from the urine into the blood...
of glucose in the proximal renal tubuli
Proximal tubule
The proximal tubule is the portion of the duct system of the nephron of the kidney which leads from Bowman's capsule to the loop of Henle.-Structure and appearance:...
is incomplete, and part of the glucose remains in the urine
Urine
Urine is a typically sterile liquid by-product of the body that is secreted by the kidneys through a process called urination and excreted through the urethra. Cellular metabolism generates numerous by-products, many rich in nitrogen, that require elimination from the bloodstream...
(glycosuria
Glycosuria
Glycosuria or glucosuria is the excretion of glucose into the urine. Ordinarily, urine contains no glucose because the kidneys are able to reclaim all of the filtered glucose back into the bloodstream. Glycosuria is nearly always caused by elevated blood glucose levels, most commonly due to...
). This increases the osmotic pressure
Osmotic pressure
Osmotic pressure is the pressure which needs to be applied to a solution to prevent the inward flow of water across a semipermeable membrane....
of the urine and inhibits reabsorption of water by the kidney, resulting in increased urine production (polyuria
Polyuria
Polyuria is a condition usually defined as excessive or abnormally large production or passage of urine . Frequent urination is sometimes included by definition, but is nonetheless usually an accompanying symptom...
) and increased fluid loss. Lost blood volume will be replaced osmotically from water held in body cells and other body compartments, causing dehydration
Dehydration
In physiology and medicine, dehydration is defined as the excessive loss of body fluid. It is literally the removal of water from an object; however, in physiological terms, it entails a deficiency of fluid within an organism...
and increased thirst.
Diagnosis
Diabetes mellitus is characterized by recurrent or persistent hyperglycemia, and is diagnosed by demonstrating any one of the following:- Fasting plasma glucose level ≥ 7.0 mmol/L (126 mg/dL).
- Plasma glucose ≥ 11.1 mmol/L (200 mg/dL) two hours after a 75 g oral glucose load as in a glucose tolerance testGlucose tolerance testA glucose tolerance test is a medical test in which glucose is given and blood samples taken afterward to determine how quickly it is cleared from the blood. The test is usually used to test for diabetes, insulin resistance, and sometimes reactive hypoglycemia and acromegaly, or rarer disorders of...
. - Symptoms of hyperglycemia and casual plasma glucose ≥ 11.1 mmol/L (200 mg/dL).
- Glycated hemoglobin (Hb A1C) ≥ 6.5%.
A positive result, in the absence of unequivocal hyperglycemia, should be confirmed by a repeat of any of the above-listed methods on a different day. It is preferable to measure a fasting glucose level because of the ease of measurement and the considerable time commitment of formal glucose tolerance testing, which takes two hours to complete and offers no prognostic advantage over the fasting test. According to the current definition, two fasting glucose measurements above 126 mg/dL (7.0 mmol/L) is considered diagnostic for diabetes mellitus.
People with fasting glucose levels from 100 to 125 mg/dL (5.6 to 6.9 mmol/L) are considered to have impaired fasting glucose. Patients with plasma glucose at or above 140 mg/dL (7.8 mmol/L), but not over 200 mg/dL (11.1 mmol/L), two hours after a 75 g oral glucose load are considered to have impaired glucose tolerance
Impaired glucose tolerance
Impaired glucose tolerance is a pre-diabetic state of dysglycemia that is associated with insulin resistance and increased risk of cardiovascular pathology. IGT may precede type 2 diabetes mellitus by many years...
. Of these two pre-diabetic states, the latter in particular is a major risk factor for progression to full-blown diabetes mellitus as well as cardiovascular disease.
Glycated hemoglobin is better than fasting glucose for determining risks of cardiovascular disease and death from any cause.
Management
Diabetes mellitus is a chronic disease which cannot be cured except in very specific situations. Management concentrates on keeping blood sugar levels as close to normal ("euglycemia") as possible, without causing hypoglycemia. This can usually be accomplished with diet, exercise, and use of appropriate medications (insulin in the case of type 1 diabetes, oral medications as well as possibly insulin in type 2 diabetes).Patient education, understanding, and participation is vital since the complications of diabetes are far less common and less severe in people who have well-managed blood sugar levels. The goal of treatment is an HbA1C level of 6.5%, but should not be lower than that, and may be set higher. Attention is also paid to other health problems that may accelerate the deleterious effects of diabetes. These include smoking
Tobacco smoking
Tobacco smoking is the practice where tobacco is burned and the resulting smoke is inhaled. The practice may have begun as early as 5000–3000 BCE. Tobacco was introduced to Eurasia in the late 16th century where it followed common trade routes...
, elevated cholesterol
Hypercholesterolemia
Hypercholesterolemia is the presence of high levels of cholesterol in the blood. It is not a disease but a metabolic derangement that can be caused by many diseases, notably cardiovascular disease...
levels, obesity
Obesity
Obesity is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health, leading to reduced life expectancy and/or increased health problems...
, high blood pressure
Hypertension
Hypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
, and lack of regular exercise.
Lifestyle
There are roles for patient education, dietetic support, sensible exercise, with the goal of keeping both short-term and long-term blood glucose levels within acceptable bounds. In addition, given the associated higher risks of cardiovascular disease, lifestyle modifications are recommended to control blood pressure.Medications
Oral medicationsMetformin
Metformin
Metformin is an oral antidiabetic drug in the biguanide class. It is the first-line drug of choice for the treatment of type 2 diabetes, in particular, in overweight and obese people and those with normal kidney function. Its use in gestational diabetes has been limited by safety concerns...
is generally recommended as a first line treatment for type 2 diabetes as there is good evidence that it decreases mortality. Routine use of aspirin
Aspirin
Aspirin , also known as acetylsalicylic acid , is a salicylate drug, often used as an analgesic to relieve minor aches and pains, as an antipyretic to reduce fever, and as an anti-inflammatory medication. It was discovered by Arthur Eichengrun, a chemist with the German company Bayer...
however has not been found to improve outcomes in uncomplicated diabetes.
Insulin
Type 1 diabetes is typically treated with a combinations of regular and NPH insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
, or synthetic insulin analogs. When insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
is used in type 2 diabetes, a long-acting formulation is usually added initially, while continuing oral medications. Doses of insulin are then increased to effect.
Support
In countries using a general practitionerGeneral practitioner
A general practitioner is a medical practitioner who treats acute and chronic illnesses and provides preventive care and health education for all ages and both sexes. They have particular skills in treating people with multiple health issues and comorbidities...
system, such as the United Kingdom
United Kingdom
The United Kingdom of Great Britain and Northern IrelandIn the United Kingdom and Dependencies, other languages have been officially recognised as legitimate autochthonous languages under the European Charter for Regional or Minority Languages...
, care may take place mainly outside hospitals, with hospital-based specialist care used only in case of complications, difficult blood sugar control, or research projects. In other circumstances, general practitioners and specialists share care of a patient in a team approach. Optometrists
Optometry
Optometry is a health care profession concerned with eyes and related structures, as well as vision, visual systems, and vision information processing in humans. Optometrists, or Doctors of Optometry, are state licensed medical professionals trained to prescribe and fit lenses to improve vision,...
, podiatrists
Podiatry
Podiatry is a branch of medicine devoted to the study, diagnosis, and treatment of disorders of the foot, ankle, and lower leg. The term podiatry came into use first in the early 20th century United States, where it now denotes a Doctor of Podiatric Medicine , a specialist who is qualified by their...
/chiropodists, dietitian
Dietitian
Dietitians supervise the preparation and service of food, develop modified diets, participate in research, and educate individuals and groups on good nutritional habits. The goals of dietitians are to provide medical nutritional intervention, and to obtain, safely prepare, serve and advise on...
s, physiotherapists
Physical therapy
Physical therapy , often abbreviated PT, is a health care profession. Physical therapy is concerned with identifying and maximizing quality of life and movement potential within the spheres of promotion, prevention, diagnosis, treatment/intervention,and rehabilitation...
, nursing specialists (e.g., DSNs (Diabetic Specialist Nurse)), nurse practitioner
Nurse practitioner
A Nurse Practitioner is an Advanced practice registered nurse who has completed graduate-level education . Additional APRN roles include the Certified Registered Nurse Anesthetist s, CNMs, and CNSs...
s, or certified diabetes educator
Certified diabetes educator
A certified diabetes educator is a health care professional who is specialized and certified to teach people with diabetes how to manage their condition....
s, may jointly provide multidisciplinary expertise.
Epidemiology
In 2000, according to the World Health Organization, at least 171 million people worldwide suffer from diabetes, or 2.8% of the population. Its incidence is increasing rapidly, and it is estimated that by 2030, this number will almost double. Diabetes mellitus occurs throughout the world, but is more common (especially type 2) in the more developed countries. The greatest increase in prevalence is, however, expected to occur in Asia and Africa, where most patients will probably be found by 2030. The increase in incidence of diabetes in developing countries follows the trend of urbanization and lifestyle changes, perhaps most importantly a "Western-style" diet. This has suggested an environmental (i.e., dietary) effect, but there is little understanding of the mechanism(s) at present, though there is much speculation, some of it most compellingly presented.Prevalence in the United States
For at least 20 years, diabetes rates in North America have been increasing substantially. In 2010 nearly 26 million people have diabetes in the United States alone, from those 7 million people remain undiagnosed. Another 57 million people are estimated to have pre-diabetes.
The Centers for Disease Control has termed the change an epidemic
Epidemic
In epidemiology, an epidemic , occurs when new cases of a certain disease, in a given human population, and during a given period, substantially exceed what is expected based on recent experience...
. The National Diabetes Information Clearinghouse estimates that diabetes costs $132 billion in the United States alone every year. About 5%–10% of diabetes cases in North America are type 1, with the rest being type 2. The fraction of type 1 in other parts of the world differs. Most of this difference is not currently understood. The American Diabetes Association cite the 2003 assessment of the National Center for Chronic Disease Prevention and Health Promotion (Centers for Disease Control and Prevention) that 1 in 3 Americans born after 2000 will develop diabetes in their lifetime.
According to the American Diabetes Association, approximately 18.3% (8.6 million) of Americans age 60 and older have diabetes. Diabetes mellitus prevalence increases with age, and the numbers of older persons with diabetes are expected to grow as the elderly population increases in number. The National Health and Nutrition Examination Survey (NHANES III) demonstrated that, in the population over 65 years old, 18% to 20% have diabetes, with 40% having either diabetes or its precursor form of impaired glucose tolerance
Impaired glucose tolerance
Impaired glucose tolerance is a pre-diabetic state of dysglycemia that is associated with insulin resistance and increased risk of cardiovascular pathology. IGT may precede type 2 diabetes mellitus by many years...
.
Prevalence in Australia
Indigenous populations in first world countries have a higher prevalence and increasing incidence of diabetes than their corresponding non-indigenous populations. In Australia the age-standardised prevalence of self-reported diabetes in Indigenous Australians is almost 4 times that of non-indigenous Australians. Preventative community health programs such as Sugar Man (diabetes education)
Sugar Man (diabetes education)
The Sugar Man is an innovative interactive model for diabetes education developed by registered nurse Michael Porter. It was first presented at Leigh Creek Hospital in South Australia and has since been used at numerous events around Australia - in particular CrocFest and some of the Healthy for...
are showing some success in tackling this problem.
Etymology
The word “diabetes” (icon or ˌ) comes from LatinLatin
Latin is an Italic language originally spoken in Latium and Ancient Rome. It, along with most European languages, is a descendant of the ancient Proto-Indo-European language. Although it is considered a dead language, a number of scholars and members of the Christian clergy speak it fluently, and...
diabētēs, which in turn comes from Ancient Greek
Ancient Greek
Ancient Greek is the stage of the Greek language in the periods spanning the times c. 9th–6th centuries BC, , c. 5th–4th centuries BC , and the c. 3rd century BC – 6th century AD of ancient Greece and the ancient world; being predated in the 2nd millennium BC by Mycenaean Greek...
διαβήτης (diabētēs) which literally means “a passer through; a siphon
Siphon
The word siphon is sometimes used to refer to a wide variety of devices that involve the flow of liquids through tubes. But in the English language today, the word siphon usually refers to a tube in an inverted U shape which causes a liquid to flow uphill, above the surface of the reservoir,...
.” Ancient Greek
Ancient Greece
Ancient Greece is a civilization belonging to a period of Greek history that lasted from the Archaic period of the 8th to 6th centuries BC to the end of antiquity. Immediately following this period was the beginning of the Early Middle Ages and the Byzantine era. Included in Ancient Greece is the...
physician
Physician
A physician is a health care provider who practices the profession of medicine, which is concerned with promoting, maintaining or restoring human health through the study, diagnosis, and treatment of disease, injury and other physical and mental impairments...
Aretaeus of Cappadocia
Aretaeus of Cappadocia
Aretaeus , is one of the most celebrated of the ancient Greek physicians, of whose life, however, few particulars are known. There is some uncertainty regarding both his age and country, but it seems probable that he practised in the 1st century CE, during the reign of Nero or Vespasian...
(fl.
Floruit
Floruit , abbreviated fl. , is a Latin verb meaning "flourished", denoting the period of time during which something was active...
1st century CE
Common Era
Common Era ,abbreviated as CE, is an alternative designation for the calendar era originally introduced by Dionysius Exiguus in the 6th century, traditionally identified with Anno Domini .Dates before the year 1 CE are indicated by the usage of BCE, short for Before the Common Era Common Era...
) used that word, with the intended meaning “excessive discharge of urine,” as the name for the disease. Ultimately, the word comes from Greek διαβαίνειν (diabainein), meaning “to pass through,” which is composed of δια- (dia-), meaning “through” and βαίνειν (bainein), meaning “to go”. The word “diabetes” is first recorded in English, in the form diabete, in a medical text written around 1425.
The word “mellitus” (m or ˈ) comes from the classical Latin word mellītus, meaning “mellite” (i.e. sweetened with honey; honey-sweet). The Latin word comes from mell-, which comes from mel, meaning “honey; sweetness; pleasant thing,” and the suffix -ītus, whose meaning is the same as that of the English suffix “-ite.” It was Thomas Willis
Thomas Willis
Thomas Willis was an English doctor who played an important part in the history of anatomy, neurology and psychiatry. He was a founding member of the Royal Society.-Life:...
who in 1675 added “mellitus” to the word “diabetes” as a designation for the disease, when he noticed that the urine of a diabetic had a sweet taste (glycosuria
Glycosuria
Glycosuria or glucosuria is the excretion of glucose into the urine. Ordinarily, urine contains no glucose because the kidneys are able to reclaim all of the filtered glucose back into the bloodstream. Glycosuria is nearly always caused by elevated blood glucose levels, most commonly due to...
). This sweet taste had been noticed in urine by the ancient Greeks, Chinese, Egyptians, Indians, and Persians.
History
Diabetes is one of the oldest known diseases. An Egyptian manuscript from c.Circa
Circa , usually abbreviated c. or ca. , means "approximately" in the English language, usually referring to a date...
1550 BCE
Common Era
Common Era ,abbreviated as CE, is an alternative designation for the calendar era originally introduced by Dionysius Exiguus in the 6th century, traditionally identified with Anno Domini .Dates before the year 1 CE are indicated by the usage of BCE, short for Before the Common Era Common Era...
mentions the phrase “the passing of too much urine.” The great Indian physician Sushruta (fl.
Floruit
Floruit , abbreviated fl. , is a Latin verb meaning "flourished", denoting the period of time during which something was active...
6th century BCE
Common Era
Common Era ,abbreviated as CE, is an alternative designation for the calendar era originally introduced by Dionysius Exiguus in the 6th century, traditionally identified with Anno Domini .Dates before the year 1 CE are indicated by the usage of BCE, short for Before the Common Era Common Era...
) identified the disease and classified it as Medhumeha. He further identified it with obesity
Obesity
Obesity is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health, leading to reduced life expectancy and/or increased health problems...
and sedentary lifestyle, advising exercises to help "cure" it. The ancient India
India
India , officially the Republic of India , is a country in South Asia. It is the seventh-largest country by geographical area, the second-most populous country with over 1.2 billion people, and the most populous democracy in the world...
ns tested for diabetes by observing whether ant
Ant
Ants are social insects of the family Formicidae and, along with the related wasps and bees, belong to the order Hymenoptera. Ants evolved from wasp-like ancestors in the mid-Cretaceous period between 110 and 130 million years ago and diversified after the rise of flowering plants. More than...
s were attracted to a person's urine, and called the ailment "sweet urine disease" (Madhumeha).
Concerning the sweetness of urine, it is to be noted that the Chinese, Japanese and Korean words for diabetes are based on the same ideographs (糖尿病) which mean "sugar urine disease". It was in 1776 that Matthew Dobson confirmed that the sweet taste comes from an excess of a kind of sugar in the urine and blood.
The first complete clinical description of diabetes was given by the Ancient Greek
Ancient Greece
Ancient Greece is a civilization belonging to a period of Greek history that lasted from the Archaic period of the 8th to 6th centuries BC to the end of antiquity. Immediately following this period was the beginning of the Early Middle Ages and the Byzantine era. Included in Ancient Greece is the...
physician
Physician
A physician is a health care provider who practices the profession of medicine, which is concerned with promoting, maintaining or restoring human health through the study, diagnosis, and treatment of disease, injury and other physical and mental impairments...
Aretaeus of Cappadocia
Aretaeus of Cappadocia
Aretaeus , is one of the most celebrated of the ancient Greek physicians, of whose life, however, few particulars are known. There is some uncertainty regarding both his age and country, but it seems probable that he practised in the 1st century CE, during the reign of Nero or Vespasian...
(fl.
Floruit
Floruit , abbreviated fl. , is a Latin verb meaning "flourished", denoting the period of time during which something was active...
1st century CE
Common Era
Common Era ,abbreviated as CE, is an alternative designation for the calendar era originally introduced by Dionysius Exiguus in the 6th century, traditionally identified with Anno Domini .Dates before the year 1 CE are indicated by the usage of BCE, short for Before the Common Era Common Era...
), who noted the excessive amount of urine which passed through the kidneys and gave the disease the name “diabetes.”
Diabetes mellitus appears to have been a death sentence in the ancient era. Hippocrates makes no mention of it, which may indicate that he felt the disease was incurable. Aretaeus did attempt to treat it but could not give a good prognosis; he commented that "life (with diabetes) is short, disgusting and painful."
In medieval Persia
History of Iran
The history of Iran has been intertwined with the history of a larger historical region, comprising the area from the Danube River in the west to the Indus River and Jaxartes in the east and from the Caucasus, Caspian Sea, and Aral Sea in the north to the Persian Gulf and the Gulf of Oman and Egypt...
, Avicenna
Avicenna
Abū ʿAlī al-Ḥusayn ibn ʿAbd Allāh ibn Sīnā , commonly known as Ibn Sīnā or by his Latinized name Avicenna, was a Persian polymath, who wrote almost 450 treatises on a wide range of subjects, of which around 240 have survived...
(980–1037) provided a detailed account on diabetes mellitus in The Canon of Medicine
The Canon of Medicine
The Canon of Medicine is an encyclopedia of Galenic medicine in five books compiled by Ibn Sīnā and completed in 1025. It presents a clear and organized summary of all the medical knowledge of the time...
, "describing the abnormal appetite and the collapse of sexual functions," and he documented the sweet taste of diabetic urine. Like Aretaeus before him, Avicenna recognized a primary and secondary diabetes. He also described diabetic gangrene
Gangrene
Gangrene is a serious and potentially life-threatening condition that arises when a considerable mass of body tissue dies . This may occur after an injury or infection, or in people suffering from any chronic health problem affecting blood circulation. The primary cause of gangrene is reduced blood...
, and treated diabetes using a mixture of lupin
Lupin
Lupinus, commonly known as Lupins or lupines , is a genus in the legume family . The genus comprises about 280 species , with major centers of diversity in South and western North America , and the Andes and secondary centers in the Mediterranean region and Africa Lupinus, commonly known as Lupins...
e, trigonella
Trigonella
Trigonella is a genus from the family Fabaceae. The best known member is the herb Fenugreek.-Species:The genus Trigonella currently has 37 recognized species:* Trigonella anguina Delile* Trigonella arabica Delile...
(fenugreek
Fenugreek
Fenugreek is a plant in the family Fabaceae. Fenugreek is used both as a herb and as a spice . The leaves and sprouts are also eaten as vegetables...
), and zedoary
Zedoary
Zedoary is the name for a perennial herb and member of the genus Curcuma Linn., family Zingiberaceae. The plant is native to India and Indonesia...
seed, which produces a considerable reduction in the excretion of sugar, a treatment which is still prescribed in modern times. Avicenna also "described diabetes insipidus very precisely for the first time", though it was later Johann Peter Frank
Johann Peter Frank
Johann Peter Frank was a German physician and hygienist who was a native of Rodalben.He studied medicine at the Universities of Strasbourg and Heidelberg, and earned his medical doctorate in 1766. He was professor at the Universities of Pavia and Göttingen, and for a period of time was personal...
(1745–1821) who first differentiated between diabetes mellitus and diabetes insipidus.
Although diabetes has been recognized since antiquity
Ancient history
Ancient history is the study of the written past from the beginning of recorded human history to the Early Middle Ages. The span of recorded history is roughly 5,000 years, with Cuneiform script, the oldest discovered form of coherent writing, from the protoliterate period around the 30th century BC...
, and treatments of various efficacy have been known in various regions since the Middle Ages
Middle Ages
The Middle Ages is a periodization of European history from the 5th century to the 15th century. The Middle Ages follows the fall of the Western Roman Empire in 476 and precedes the Early Modern Era. It is the middle period of a three-period division of Western history: Classic, Medieval and Modern...
, and in legend
Snake oil
Snake oil is a topical preparation made from the Chinese Water Snake , which is used to treat joint pain. However, the most common usage of the phrase is as a derogatory term for quack medicine...
for much longer, pathogenesis of diabetes has only been understood experimentally since about 1900.
The discovery of a role for the pancreas in diabetes is generally ascribed to Joseph von Mering
Joseph von Mering
Josef, Baron von Mering was a German physician.Working at the University of Strasbourg, Mering was the first person to discover that one of the pancreatic functions is the production of insulin, a hormone which controls blood sugar levels.Mering was curious about the...
and Oskar Minkowski
Oskar Minkowski
Oskar Minkowski He held a professor at at the University of Breslau and is most famous for his research on diabetes...
, who in 1889 found that dogs whose pancreas was removed developed all the signs and symptoms of diabetes and died shortly afterwards.
In 1910, Sir Edward Albert Sharpey-Schafer suggested that people with diabetes were deficient in a single chemical that was normally produced by the pancreas—he proposed calling this substance insulin, from the Latin insula, meaning island, in reference to the insulin-producing islets of Langerhans
Islets of Langerhans
The islets of Langerhans are the regions of the pancreas that contain its endocrine cells. Discovered in 1869 by German pathological anatomist Paul Langerhans at the age of 22, the islets of Langerhans constitute approximately 1 to 2% of the mass of the pancreas...
in the pancreas.
The endocrine role of the pancreas in metabolism, and indeed the existence of insulin, was not further clarified until 1921, when Sir Frederick Grant Banting and Charles Herbert Best repeated the work of Von Mering and Minkowski, and went further to demonstrate they could reverse induced diabetes in dogs by giving them an extract from the pancreatic islets of Langerhans of healthy dogs.
Banting, Best, and colleagues (especially the chemist Collip
James Collip
James Bertram Collip, Ph.D. was part of the Toronto group which isolated insulin. He served as the Chair of the Department of Biochemistry at McGill University from 1928-1941 and Dean of Medicine at the University of Western Ontario from 1947-1961, where he was a charter member of The Kappa Alpha...
) went on to purify the hormone insulin from bovine pancreases at the University of Toronto
University of Toronto
The University of Toronto is a public research university in Toronto, Ontario, Canada, situated on the grounds that surround Queen's Park. It was founded by royal charter in 1827 as King's College, the first institution of higher learning in Upper Canada...
. This led to the availability of an effective treatment—insulin injections—and the first patient was treated in 1922. For this, Banting and laboratory director MacLeod received the Nobel Prize in Physiology or Medicine
Nobel Prize in Physiology or Medicine
The Nobel Prize in Physiology or Medicine administered by the Nobel Foundation, is awarded once a year for outstanding discoveries in the field of life science and medicine. It is one of five Nobel Prizes established in 1895 by Swedish chemist Alfred Nobel, the inventor of dynamite, in his will...
in 1923; both shared their Prize money with others in the team who were not recognized, in particular Best and Collip. Banting and Best made the patent available without charge and did not attempt to control commercial production. Insulin
Insulin
Insulin is a hormone central to regulating carbohydrate and fat metabolism in the body. Insulin causes cells in the liver, muscle, and fat tissue to take up glucose from the blood, storing it as glycogen in the liver and muscle....
production and therapy rapidly spread around the world, largely as a result of this decision. Banting is honored by World Diabetes Day
World Diabetes Day
World Diabetes Day is the primary global awareness campaign of the diabetes mellitus world and is held on November 14 of each year. It was introduced in 1991 by the International Diabetes Federation and the World Health Organization in response to the alarming rise of diabetes around the world...
which is held on his birthday, November 14.
The distinction between what is now known as type 1 diabetes and type 2 diabetes was first clearly made by Sir Harold Percival (Harry) Himsworth
Harold Percival Himsworth
Sir Harold Percival Himsworth, KCB was a British scientist, best known for his medical research on diabetes mellitus.-Early life:...
, and published in January 1936.
Despite the availability of treatment, diabetes has remained a major cause of death. For instance, statistics
Statistics
Statistics is the study of the collection, organization, analysis, and interpretation of data. It deals with all aspects of this, including the planning of data collection in terms of the design of surveys and experiments....
reveal that the cause-specific mortality rate
Mortality rate
Mortality rate is a measure of the number of deaths in a population, scaled to the size of that population, per unit time...
during 1927 amounted to about 47.7 per 100,000 population in Malta
Malta
Malta , officially known as the Republic of Malta , is a Southern European country consisting of an archipelago situated in the centre of the Mediterranean, south of Sicily, east of Tunisia and north of Libya, with Gibraltar to the west and Alexandria to the east.Malta covers just over in...
.
Other landmark discoveries include:
- Identification of the first of the sulfonylureaSulfonylureaSulfonylurea derivatives are a class of antidiabetic drugs that are used in the management of diabetes mellitus type 2. They act by increasing insulin release from the beta cells in the pancreas.-First generation:* Carbutamide...
s in 1942 - Reintroduction of the use of biguanides for Type 2 diabetes in the late 1950s. The initial phenforminPhenforminPhenformin is an anti-diabetic drug from the biguanide class. It was marketed as DBI by Ciba-Geigy but was withdrawn from most markets in the late 1970s due to a high risk of lactic acidosis, which was fatal in 50% of cases....
was withdrawn worldwide (in the U.S. in 1977) due to its potential for sometimes fatal lactic acidosis and metforminMetforminMetformin is an oral antidiabetic drug in the biguanide class. It is the first-line drug of choice for the treatment of type 2 diabetes, in particular, in overweight and obese people and those with normal kidney function. Its use in gestational diabetes has been limited by safety concerns...
was first marketed in France in 1979, but not until 1994 in the US. - The determination of the amino acid sequence of insulin (by Sir Frederick SangerFrederick SangerFrederick Sanger, OM, CH, CBE, FRS is an English biochemist and a two-time Nobel laureate in chemistry, the only person to have been so. In 1958 he was awarded a Nobel prize in chemistry "for his work on the structure of proteins, especially that of insulin"...
, for which he received a Nobel Prize) - The radioimmunoassayRadioimmunoassayRadioimmunoassay is a very sensitive in vitro assay technique used to measure concentrations of antigens by use of antibodies...
for insulin, as discovered by Rosalyn Yalow and Solomon BersonSolomon BersonSolomon Aaron Berson was an American physician and scientist whose discoveries, mostly together with Rosalyn Yalow, caused major advances in clinical biochemistry....
(gaining Yalow the 1977 Nobel Prize in Physiology or Medicine) - The three-dimensional structure of insulin
- Dr Gerald ReavenGerald ReavenGerald M. "Jerry" Reaven is an American endocrinologist and professor emeritus in medicine at the Stanford University School of Medicine in Stanford, California, United States.Reaven's work on insulin resistance and diabetes with John W...
's identification of the constellation of symptoms now called metabolic syndromeMetabolic syndromeMetabolic syndrome is a combination of medical disorders that, when occurring together, increase the risk of developing cardiovascular disease and diabetes. It affects one in five people in the United States and prevalence increases with age...
in 1988 - Demonstration that intensive glycemic control in type 1 diabetes reduces chronic side effects more as glucose levels approach 'normal' in a large longitudinal study, and also in type 2 diabetics in other large studies
- Identification of the first thiazolidinedioneThiazolidinedioneThe thiazolidinediones , also known as glitazones, are a class of medications used in the treatment of diabetes mellitus type 2. They were introduced in the late 1990s.- Mechanism of action :...
as an effective insulin sensitizer during the 1990s
In 1980, U.S. biotech company Genentech developed biosynthetic human insulin. The insulin was isolated from genetically altered bacteria (the bacteria contain the human gene for synthesizing synthetic human insulin), which produce large quantities of insulin. The purified insulin is distributed to pharmacies for use by diabetes patients. Initially, this development was not regarded by the medical profession as a clinically meaningful development. However, by 1996, the advent of insulin analogues which had vastly improved absorption, distribution, metabolism, and excretion (ADME)
ADME
ADME is an acronym in pharmacokinetics and pharmacology for absorption, distribution, metabolism, and excretion, and describes the disposition of a pharmaceutical compound within an organism...
characteristics which were clinically meaningful based on this early biotechnology development.
Society and culture
The 1990 "St. Vincent DeclarationSt. Vincent Declaration
The St. Vincent Declaration is a set of goals for the medical care of people with diabetes mellitus published as the product of an international conference held in St. Vincent, Italy, on 10-12 October 1989...
" was the result of international efforts to improve the care accorded to those with diabetes. Doing so is important both in terms of quality of life and life expectancy but also economically—expenses due to diabetes have been shown to be a major drain on health-and productivity-related resources for healthcare systems and governments.
Several countries established more and less successful national diabetes programmes to improve treatment of the disease.
A study shows that diabetic patients with neuropathic symptoms such as numbness
Paresthesia
Paresthesia , spelled "paraesthesia" in British English, is a sensation of tingling, burning, pricking, or numbness of a person's skin with no apparent long-term physical effect. It is more generally known as the feeling of "pins and needles" or of a limb "falling asleep"...
or tingling in feet or hands are twice as likely to be unemployed as those without the symptoms.
In other animals
In animals, diabetes is most commonly encountered in dogs and cats. Middle-aged animals are most commonly affected. Female dogs are twice as likely to be affected as males, while according to some sources male cats are also more prone than females. In both species, all breeds may be affected, but some small dog breeds are particularly likely to develop diabetes, such as Miniature PoodlesPoodle
The Poodle is a breed of dog. The poodle breed is found officially in toy, miniature, and standard sizes, with many coat colors. Originally bred as a type of water dog, the poodle is highly intelligent and skillful in many dog sports, including agility, obedience, tracking, and even herding...
. The symptoms may relate to fluid loss and polyuria, but the course may also be insidious. Diabetic animals are more prone to infections. The long-term complications recognised in humans are much rarer in animals. The principles of treatment (weight loss, oral antidiabetics, subcutaneous insulin) and management of emergencies (e.g. ketoacidosis) are similar to those in humans.
External links
- Diabetes at the Open Directory ProjectOpen Directory ProjectThe Open Directory Project , also known as Dmoz , is a multilingual open content directory of World Wide Web links. It is owned by Netscape but it is constructed and maintained by a community of volunteer editors.ODP uses a hierarchical ontology scheme for organizing site listings...
- American Diabetes Association
- IDF Diabetes Atlas
- International Diabetes Federation
- National Diabetes Education Program
- Peers for Progress
- World Diabetes Day