

Shock
Encyclopedia
Circulatory shock, commonly known simply as shock, is a life-threatening medical condition that occurs due to inadequate substrate
for aerobic cellular respiration. In the early stages this is generally an inadequate tissue levels of oxygen
.
The typical signs of shock are low blood pressure
, a rapid heartbeat
and signs of poor end-organ perfusion
or "decompensation" (such as low urine output, confusion or loss of consciousness). There are times that a person's blood pressure may remain stable, but may still be in circulatory shock, so it is not always a symptom.
A circulatory shock should not be confused with the emotional state of shock, as the two are not related. Medical shock is a life-threatening medical emergency
and one of the most common causes of death for critically ill people. Shock can have a variety of effects, all with similar outcomes, but all relate to a problem with the body's circulatory system. For example, shock may lead to hypoxemia
(a lack of oxygen in arterial blood) or cardiac arrest
(the heart stopping).
One of the key dangers of shock is that it progresses by a positive feedback
mechanism. Once shock begins, it tends to make itself worse. This is why immediate treatment of shock is critical.
, decreased urine output, and confusion these may not always be present. While a fast heart rate is common, those on β-blockers
, those who are athletic and in 30% of cases those with shock due to intra abdominal bleeding may have a normal or slow heart rate. Specific subtypes of shock may have additional symptoms.
The severity of hemorrhagic shock can be graded on a 1-4 scale on the physical signs. This approximates to the effective loss of blood volume.
, anaphylactic, and neurogenic
causes. The SIRS features typically occur in early septic shock.
 There are four stages of shock. As it is a complex and continuous condition there is no sudden transition from one stage to the next. At a cellular level shock is oxygen demand greater than oxygen supply.
There are four stages of shock. As it is a complex and continuous condition there is no sudden transition from one stage to the next. At a cellular level shock is oxygen demand greater than oxygen supply.
. Due to the lack of oxygen, the cell membranes become damaged, they become leaky to extra-cellular fluid, and the cells perform anaerobic respiration
. This causes a build-up of lactic
and pyruvic acid
which results in systemic metabolic acidosis
. The process of removing these compounds from the cells by the liver
requires oxygen, which is absent.
, the person will begin to hyperventilate in order to rid the body of carbon dioxide (CO2). CO2 indirectly acts to acidify the blood and by removing it the body is attempting to raise the pH of the blood. The baroreceptors in the arteries
detect the resulting hypotension
, and cause the release of adrenaline and noradrenaline. Noradrenaline causes predominately vasoconstriction
with a mild increase in heart rate
, whereas adrenaline predominately causes an increase in heart rate
with a small effect on the vascular
tone; the combined effect results in an increase in blood pressure
. This is known as Cushing reflex
and its triad
is the subjective identifying characteristic of this stage. Renin
-angiotensin
axis is activated and arginine vasopressin (Anti-diuretic hormone; ADH) is released to conserve fluid via the kidneys. These hormones cause the vasoconstriction of the kidneys, gastrointestinal tract
, and other organs to divert blood to the heart, lungs and brain
. The lack of blood to the renal system causes the characteristic low urine
production. However the effects of the Renin
-angiotensin
axis take time and are of little importance to the immediate homeostatic mediation of shock.
ions build up within while potassium
ions leak out. As anaerobic metabolism continues, increasing the body's metabolic acidosis, the arteriolar smooth muscle and precapillary sphincters relax such that blood remains in the capillaries. Due to this, the hydrostatic pressure will increase and, combined with histamine
release, this will lead to leakage of fluid and protein
into the surrounding tissues. As this fluid is lost, the blood concentration and viscosity
increase, causing sludging of the micro-circulation. The prolonged vasoconstriction will also cause the vital organs to be compromised due to reduced perfusion. If the bowel becomes sufficiently ischemic, bacteria may enter the blood stream, resulting in the increased complication of endotoxic shock
.
and cell death are occurring, and death will occur imminently. One of the primary reasons that shock is irreversible at this point is that much cellular ATP
has been degraded into adenosine in the absence of oxygen as an electron receptor in the mitochondrial matrix. Adenosine easily perfuses out of cellular membranes into extracellular fluid, furthering capillary vasodilation
, and then is transformed into uric acid
. Because cells can only produce adenosine at a rate of about 2% of the cell's total need per hour, even restoring oxygen is futile at this point because there is no adenosine to phosphorylate into ATP.
followed by a decrease in mixed venous oxygen saturation (SmvO2) as measured in the pulmonary artery
via a pulmonary artery catheter
. Central venous oxygen saturation (ScvO2) as measured via a central line correlates well with SmvO2 and are easier to acquire. If shock progresses anaerobic metabolism will begin to occur with an increased blood lactic acid
as the result. While many laboratory tests are typically performed there is no test that either makes or excludes the diagnosis. A chest X-ray
or emergency department ultrasound may be useful to determine volume state.
. Its primary cause is hemorrhage or loss of fluid from the circulation
. Vomiting
and diarrhea
are the most common cause in children. With other causes including burns, environmental exposure and excess urine loss due to diabetic ketoacidosis
and diabetes insipidus
.
. Other causes of cardiogenic shock include dysrhythmia
s, cardiomyopathy
/myocarditis
, congestive heart failure
(CHF), contusio cordis, or cardiac valveproblems.
in adults and as the pathophysiology appears similar in children and other types of shock treatment this has been extrapolated to these areas. Management may include securing the airway via intubation
to decrease the work of breathing, oxygen supplementation, intravenous fluids and a passive leg raise (not Trendelenburg position
), and blood transfusions. It is important to keep the person warm as well as adequately manage pain and anxiety as these can increase oxygen consumption.
should be administered to keep the hemoglobin
greater than 100 gms/l.
For those with hemorrhagic shock the current evidence supports limiting the use of fluids for penetrating thorax and abdominal injuries allowing mild hypotension
to persist (known as permissive hypotension
). Targets include a mean arterial pressure
of 60 mmHg, a systolic blood pressure of 70-90 mmHg, or until their adequate mentation and peripheral pulses.
but may be of use in neurogenic shock
. Activated protein C (Xigris) while once aggressively promoted for the management of septic shock
has not been found to improve survival and is associated with a number of complications, thus is no longer recommended. The use of sodium bicarbonate
is controversial as it has not been shown to improve outcomes. If used at all it should only be considered if the pH is less than 7.0.
of 8-12 mmHg and a mean arterial pressure
of 65-95 mmHg. In trauma the goal is to stop the bleeding which in many cases requires surgical interventions.
Substrate
Substrate may mean:*Substrate , Natural stone, masonry surface, ceramic and porcelain tiles*Substrate , the material used in the bottom of an aquarium*Substrate , the material used in the bottom of a vivarium or terrarium...
for aerobic cellular respiration. In the early stages this is generally an inadequate tissue levels of oxygen
Oxygen
Oxygen is the element with atomic number 8 and represented by the symbol O. Its name derives from the Greek roots ὀξύς and -γενής , because at the time of naming, it was mistakenly thought that all acids required oxygen in their composition...
.
The typical signs of shock are low blood pressure
Hypotension
In physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
, a rapid heartbeat
Tachycardia
Tachycardia comes from the Greek words tachys and kardia . Tachycardia typically refers to a heart rate that exceeds the normal range for a resting heart rate...
and signs of poor end-organ perfusion
Perfusion
In physiology, perfusion is the process of nutritive delivery of arterial blood to a capillary bed in the biological tissue. The word is derived from the French verb "perfuser" meaning to "pour over or through."...
or "decompensation" (such as low urine output, confusion or loss of consciousness). There are times that a person's blood pressure may remain stable, but may still be in circulatory shock, so it is not always a symptom.
A circulatory shock should not be confused with the emotional state of shock, as the two are not related. Medical shock is a life-threatening medical emergency
Medical emergency
A medical emergency is an injury or illness that is acute and poses an immediate risk to a person's life or long term health. These emergencies may require assistance from another person, who should ideally be suitably qualified to do so, although some of these emergencies can be dealt with by the...
and one of the most common causes of death for critically ill people. Shock can have a variety of effects, all with similar outcomes, but all relate to a problem with the body's circulatory system. For example, shock may lead to hypoxemia
Hypoxemia
Hypoxemia is generally defined as decreased partial pressure of oxygen in blood, sometimes specifically as less than or causing hemoglobin oxygen saturation of less than 90%.-Distinction from anemia and hypoxia:...
(a lack of oxygen in arterial blood) or cardiac arrest
Cardiac arrest
Cardiac arrest, is the cessation of normal circulation of the blood due to failure of the heart to contract effectively...
(the heart stopping).
One of the key dangers of shock is that it progresses by a positive feedback
Positive feedback
Positive feedback is a process in which the effects of a small disturbance on a system include an increase in the magnitude of the perturbation. That is, A produces more of B which in turn produces more of A. In contrast, a system that responds to a perturbation in a way that reduces its effect is...
mechanism. Once shock begins, it tends to make itself worse. This is why immediate treatment of shock is critical.
Signs and symptoms
The presentation of shock is variable with some people having only minimal symptoms such as confusion and weakness. While the general signs for all types of shock are low blood pressureHypotension
In physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
, decreased urine output, and confusion these may not always be present. While a fast heart rate is common, those on β-blockers
Beta blocker
Beta blockers or beta-adrenergic blocking agents, beta-adrenergic antagonists, beta-adrenoreceptor antagonists or beta antagonists, are a class of drugs used for various indications. They are particularly for the management of cardiac arrhythmias, cardioprotection after myocardial infarction ,...
, those who are athletic and in 30% of cases those with shock due to intra abdominal bleeding may have a normal or slow heart rate. Specific subtypes of shock may have additional symptoms.
Hypovolemic
Direct loss of effective circulating blood volume leading to:- A rapid, weak, thready pulse due to decreased blood flow combined with tachycardia
- Cool, clammy skin due to vasoconstrictionVasoconstrictionVasoconstriction is the narrowing of the blood vessels resulting from contraction of the muscular wall of the vessels, particularly the large arteries, small arterioles and veins. The process is the opposite of vasodilation, the widening of blood vessels. The process is particularly important in...
and stimulation of vasoconstriction - Rapid and shallow respirations due to sympathetic nervous system stimulation and acidosis
- HypothermiaHypothermiaHypothermia is a condition in which core temperature drops below the required temperature for normal metabolism and body functions which is defined as . Body temperature is usually maintained near a constant level of through biologic homeostasis or thermoregulation...
due to decreased perfusion and evaporation of sweat - Thirst and dry mouth, due to fluid depletion
- Cold and mottled skin (cutis marmorataCutis marmorataWhen a newborn infant is exposed to low environmental temperatures, an evanescent, lacy, reticulated red and/or blue cutaneous vascular pattern appears over most of the body surface...
), especially extremities, due to insufficient perfusion of the skin
The severity of hemorrhagic shock can be graded on a 1-4 scale on the physical signs. This approximates to the effective loss of blood volume.
Cardiogenic
- Distended jugular veinJugular veinThe jugular veins are veins that bring deoxygenated blood from the head back to the heart via the superior vena cava.-Internal and external:There are two sets of jugular veins: external and internal....
s due to increased jugular venous pressureJugular venous pressureThe jugular venous pressure is the indirectly observed pressure over the venous system... - Weak or absent pulse
- Arrhythmia, often tachycardic
- Pulsus paradoxusPulsus paradoxusIn medicine, a pulsus paradoxus , also paradoxic pulse or paradoxical pulse, is defined as an exaggeration of the normal variation during the inspiratory phase of respiration, in which the blood pressure declines as one inhales and increases as one exhales...
in case of tamponadeCardiac tamponadeCardiac tamponade, also known as pericardial tamponade, is an emergency condition in which fluid accumulates in the pericardium ....
Distributive
Distributive shock includes infectiousSepsis
Sepsis is a potentially deadly medical condition that is characterized by a whole-body inflammatory state and the presence of a known or suspected infection. The body may develop this inflammatory response by the immune system to microbes in the blood, urine, lungs, skin, or other tissues...
, anaphylactic, and neurogenic
Neurogenic shock
Neurogenic shock is a distributive type of shock resulting in hypotension, occasionally with bradycardia, that is attributed to the disruption of the autonomic pathways within the spinal cord. Hypotension occurs due to decreased systemic vascular resistance resulting in pooling of blood within the...
causes. The SIRS features typically occur in early septic shock.
Septic shock
- Fever may occur in sepsisSepsisSepsis is a potentially deadly medical condition that is characterized by a whole-body inflammatory state and the presence of a known or suspected infection. The body may develop this inflammatory response by the immune system to microbes in the blood, urine, lungs, skin, or other tissues...
- Warm and sweaty skin due to vasodilation
Anaphylaxisis
- Hives may present on the skin
- Localised oedema, especially around the face
- Weak and rapid pulse
- Breathlessness and cough due to narrowing of airwaysBronchospasmBronchospasm or a bronchial spasm is a sudden constriction of the muscles in the walls of the bronchioles. It is caused by the release of substances from mast cells or basophils under the influence of anaphylatoxins...
and swelling of the throat
Pathophysiology
Initial
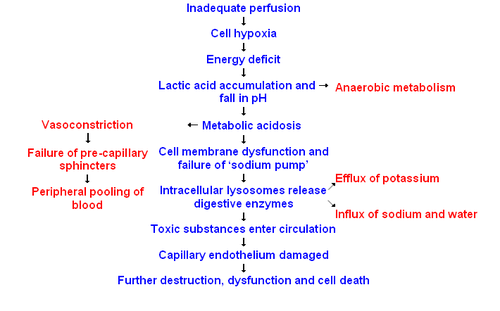
During this stage, the hypoperfusional state causes hypoxiaHypoxia (medical)
Hypoxia, or hypoxiation, is a pathological condition in which the body as a whole or a region of the body is deprived of adequate oxygen supply. Variations in arterial oxygen concentrations can be part of the normal physiology, for example, during strenuous physical exercise...
. Due to the lack of oxygen, the cell membranes become damaged, they become leaky to extra-cellular fluid, and the cells perform anaerobic respiration
Anaerobic respiration
Anaerobic respiration is a form of respiration using electron acceptors other than oxygen. Although oxygen is not used as the final electron acceptor, the process still uses a respiratory electron transport chain; it is respiration without oxygen...
. This causes a build-up of lactic
Lactic acid
Lactic acid, also known as milk acid, is a chemical compound that plays a role in various biochemical processes and was first isolated in 1780 by the Swedish chemist Carl Wilhelm Scheele. Lactic acid is a carboxylic acid with the chemical formula C3H6O3...
and pyruvic acid
Pyruvic acid
Pyruvic acid is an organic acid, a ketone, as well as the simplest of the alpha-keto acids. The carboxylate ion of pyruvic acid, CH3COCOO−, is known as pyruvate, and is a key intersection in several metabolic pathways....
which results in systemic metabolic acidosis
Metabolic acidosis
In medicine, metabolic acidosis is a condition that occurs when the body produces too much acid or when the kidneys are not removing enough acid from the body. If unchecked, metabolic acidosis leads to acidemia, i.e., blood pH is low due to increased production of hydrogen by the body or the...
. The process of removing these compounds from the cells by the liver
Liver
The liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion...
requires oxygen, which is absent.
Compensatory
This stage is characterised by the body employing physiological mechanisms, including neural, hormonal and bio-chemical mechanisms in an attempt to reverse the condition. As a result of the acidosisAcidosis
Acidosis is an increased acidity in the blood and other body tissue . If not further qualified, it usually refers to acidity of the blood plasma....
, the person will begin to hyperventilate in order to rid the body of carbon dioxide (CO2). CO2 indirectly acts to acidify the blood and by removing it the body is attempting to raise the pH of the blood. The baroreceptors in the arteries
Artery
Arteries are blood vessels that carry blood away from the heart. This blood is normally oxygenated, exceptions made for the pulmonary and umbilical arteries....
detect the resulting hypotension
Hypotension
In physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
, and cause the release of adrenaline and noradrenaline. Noradrenaline causes predominately vasoconstriction
Vasoconstriction
Vasoconstriction is the narrowing of the blood vessels resulting from contraction of the muscular wall of the vessels, particularly the large arteries, small arterioles and veins. The process is the opposite of vasodilation, the widening of blood vessels. The process is particularly important in...
with a mild increase in heart rate
Heart rate
Heart rate is the number of heartbeats per unit of time, typically expressed as beats per minute . Heart rate can vary as the body's need to absorb oxygen and excrete carbon dioxide changes, such as during exercise or sleep....
, whereas adrenaline predominately causes an increase in heart rate
Heart rate
Heart rate is the number of heartbeats per unit of time, typically expressed as beats per minute . Heart rate can vary as the body's need to absorb oxygen and excrete carbon dioxide changes, such as during exercise or sleep....
with a small effect on the vascular
Blood vessel
The blood vessels are the part of the circulatory system that transports blood throughout the body. There are three major types of blood vessels: the arteries, which carry the blood away from the heart; the capillaries, which enable the actual exchange of water and chemicals between the blood and...
tone; the combined effect results in an increase in blood pressure
Blood pressure
Blood pressure is the pressure exerted by circulating blood upon the walls of blood vessels, and is one of the principal vital signs. When used without further specification, "blood pressure" usually refers to the arterial pressure of the systemic circulation. During each heartbeat, BP varies...
. This is known as Cushing reflex
Cushing reflex
Cushing reflex is a physiological nervous system response to increased intracranial pressure that results in Cushing's triad of widening pulse pressure, irregular breathing, and a reduction of the...
and its triad
Cushing's triad
Cushing's triad is a clinical triad variably defined as either hypertension, bradycardia, andirregular respiration , or less commonly as widened pulse pressure , irregular respiration, and bradycardia...
is the subjective identifying characteristic of this stage. Renin
Renin
Renin , also known as an angiotensinogenase, is an enzyme that participates in the body's renin-angiotensin system -- also known as the Renin-Angiotensin-Aldosterone Axis -- that mediates extracellular volume , and arterial vasoconstriction...
-angiotensin
Angiotensin
Angiotensin, a peptide hormone, causes blood vessels to constrict, and drives blood pressure up. It is part of the renin-angiotensin system, which is a major target for drugs that lower blood pressure. Angiotensin also stimulates the release of aldosterone, another hormone, from the adrenal cortex...
axis is activated and arginine vasopressin (Anti-diuretic hormone; ADH) is released to conserve fluid via the kidneys. These hormones cause the vasoconstriction of the kidneys, gastrointestinal tract
Gastrointestinal tract
The human gastrointestinal tract refers to the stomach and intestine, and sometimes to all the structures from the mouth to the anus. ....
, and other organs to divert blood to the heart, lungs and brain
Brain
The brain is the center of the nervous system in all vertebrate and most invertebrate animals—only a few primitive invertebrates such as sponges, jellyfish, sea squirts and starfishes do not have one. It is located in the head, usually close to primary sensory apparatus such as vision, hearing,...
. The lack of blood to the renal system causes the characteristic low urine
Urine
Urine is a typically sterile liquid by-product of the body that is secreted by the kidneys through a process called urination and excreted through the urethra. Cellular metabolism generates numerous by-products, many rich in nitrogen, that require elimination from the bloodstream...
production. However the effects of the Renin
Renin
Renin , also known as an angiotensinogenase, is an enzyme that participates in the body's renin-angiotensin system -- also known as the Renin-Angiotensin-Aldosterone Axis -- that mediates extracellular volume , and arterial vasoconstriction...
-angiotensin
Angiotensin
Angiotensin, a peptide hormone, causes blood vessels to constrict, and drives blood pressure up. It is part of the renin-angiotensin system, which is a major target for drugs that lower blood pressure. Angiotensin also stimulates the release of aldosterone, another hormone, from the adrenal cortex...
axis take time and are of little importance to the immediate homeostatic mediation of shock.
Progressive
Should the cause of the crisis not be successfully treated, the shock will proceed to the progressive stage and the compensatory mechanisms begin to fail. Due to the decreased perfusion of the cells, sodiumSodium
Sodium is a chemical element with the symbol Na and atomic number 11. It is a soft, silvery-white, highly reactive metal and is a member of the alkali metals; its only stable isotope is 23Na. It is an abundant element that exists in numerous minerals, most commonly as sodium chloride...
ions build up within while potassium
Potassium
Potassium is the chemical element with the symbol K and atomic number 19. Elemental potassium is a soft silvery-white alkali metal that oxidizes rapidly in air and is very reactive with water, generating sufficient heat to ignite the hydrogen emitted in the reaction.Potassium and sodium are...
ions leak out. As anaerobic metabolism continues, increasing the body's metabolic acidosis, the arteriolar smooth muscle and precapillary sphincters relax such that blood remains in the capillaries. Due to this, the hydrostatic pressure will increase and, combined with histamine
Histamine
Histamine is an organic nitrogen compound involved in local immune responses as well as regulating physiological function in the gut and acting as a neurotransmitter. Histamine triggers the inflammatory response. As part of an immune response to foreign pathogens, histamine is produced by...
release, this will lead to leakage of fluid and protein
Protein
Proteins are biochemical compounds consisting of one or more polypeptides typically folded into a globular or fibrous form, facilitating a biological function. A polypeptide is a single linear polymer chain of amino acids bonded together by peptide bonds between the carboxyl and amino groups of...
into the surrounding tissues. As this fluid is lost, the blood concentration and viscosity
Viscosity
Viscosity is a measure of the resistance of a fluid which is being deformed by either shear or tensile stress. In everyday terms , viscosity is "thickness" or "internal friction". Thus, water is "thin", having a lower viscosity, while honey is "thick", having a higher viscosity...
increase, causing sludging of the micro-circulation. The prolonged vasoconstriction will also cause the vital organs to be compromised due to reduced perfusion. If the bowel becomes sufficiently ischemic, bacteria may enter the blood stream, resulting in the increased complication of endotoxic shock
Septic shock
Septic shock is a medical emergency caused by decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis, though the microbe may be systemic or localized to a particular site. It can cause multiple organ dysfunction syndrome and death...
.
Refractory
At this stage, the vital organs have failed and the shock can no longer be reversed. Brain damageBrain damage
"Brain damage" or "brain injury" is the destruction or degeneration of brain cells. Brain injuries occur due to a wide range of internal and external factors...
and cell death are occurring, and death will occur imminently. One of the primary reasons that shock is irreversible at this point is that much cellular ATP
Adenosine triphosphate
Adenosine-5'-triphosphate is a multifunctional nucleoside triphosphate used in cells as a coenzyme. It is often called the "molecular unit of currency" of intracellular energy transfer. ATP transports chemical energy within cells for metabolism...
has been degraded into adenosine in the absence of oxygen as an electron receptor in the mitochondrial matrix. Adenosine easily perfuses out of cellular membranes into extracellular fluid, furthering capillary vasodilation
Vasodilation
Vasodilation refers to the widening of blood vessels resulting from relaxation of smooth muscle cells within the vessel walls, particularly in the large arteries, smaller arterioles and large veins. The process is essentially the opposite of vasoconstriction, or the narrowing of blood vessels. When...
, and then is transformed into uric acid
Uric acid
Uric acid is a heterocyclic compound of carbon, nitrogen, oxygen, and hydrogen with the formula C5H4N4O3. It forms ions and salts known as urates and acid urates such as ammonium acid urate. Uric acid is created when the body breaks down purine nucleotides. High blood concentrations of uric acid...
. Because cells can only produce adenosine at a rate of about 2% of the cell's total need per hour, even restoring oxygen is futile at this point because there is no adenosine to phosphorylate into ATP.
Septic shock
- Systemic leukocyte adhesion to endothelial tissue
- Reduced contractility of the heart
- Activation of the coagulation pathways, resulting in disseminated intravascular coagulationDisseminated intravascular coagulationDisseminated intravascular coagulation , also known as disseminated intravascular coagulopathy or consumptive coagulopathy, is a pathological activation of coagulation mechanisms that happens in response to a variety of diseases. DIC leads to the formation of small blood clots inside the blood...
- Increased levels of neutrophils
Diagnosis
The first changes seen in shock is an increased cardiac outputCardiac output
Cardiac output is the volume of blood being pumped by the heart, in particular by a left or right ventricle in the time interval of one minute. CO may be measured in many ways, for example dm3/min...
followed by a decrease in mixed venous oxygen saturation (SmvO2) as measured in the pulmonary artery
Pulmonary artery
The pulmonary arteries carry deoxygenated blood from the heart to the lungs. They are the only arteries that carry deoxygenated blood....
via a pulmonary artery catheter
Pulmonary artery catheter
In medicine pulmonary artery catheterization is the insertion of a catheter into a pulmonary artery. Its purpose is diagnostic; it is used to detect heart failure or sepsis, monitor therapy, and evaluate the effects of drugs...
. Central venous oxygen saturation (ScvO2) as measured via a central line correlates well with SmvO2 and are easier to acquire. If shock progresses anaerobic metabolism will begin to occur with an increased blood lactic acid
Lactic acid
Lactic acid, also known as milk acid, is a chemical compound that plays a role in various biochemical processes and was first isolated in 1780 by the Swedish chemist Carl Wilhelm Scheele. Lactic acid is a carboxylic acid with the chemical formula C3H6O3...
as the result. While many laboratory tests are typically performed there is no test that either makes or excludes the diagnosis. A chest X-ray
Chest X-ray
In medicine, a chest radiograph, commonly called a chest X-ray , is a projection radiograph of the chest used to diagnose conditions affecting the chest, its contents, and nearby structures...
or emergency department ultrasound may be useful to determine volume state.
Differential diagnosis
Shock is a common end point of many medical conditions. It has been divided into four main types based on the underlying cause: hypovolemic, distributive, cardiogenic and obstructive. A few additional classifications are occasionally used including: endocrinologic shock.Hypovolemic
This is the most common type of shock and is caused by insufficient circulating volumeBlood volume
Blood volume is the volume of blood in the circulatory system of an individual.-Humans:A typical adult has a blood volume of approximately between 4.7 and 5 liters, with females generally having less blood volume than males....
. Its primary cause is hemorrhage or loss of fluid from the circulation
Circulatory system
The circulatory system is an organ system that passes nutrients , gases, hormones, blood cells, etc...
. Vomiting
Vomiting
Vomiting is the forceful expulsion of the contents of one's stomach through the mouth and sometimes the nose...
and diarrhea
Diarrhea
Diarrhea , also spelled diarrhoea, is the condition of having three or more loose or liquid bowel movements per day. It is a common cause of death in developing countries and the second most common cause of infant deaths worldwide. The loss of fluids through diarrhea can cause dehydration and...
are the most common cause in children. With other causes including burns, environmental exposure and excess urine loss due to diabetic ketoacidosis
Diabetic ketoacidosis
Diabetic ketoacidosis is a potentially life-threatening complication in patients with diabetes mellitus. It happens predominantly in those with type 1 diabetes, but it can occur in those with type 2 diabetes under certain circumstances...
and diabetes insipidus
Diabetes insipidus
Diabetes insipidus is a condition characterized by excessive thirst and excretion of large amounts of severely diluted urine, with reduction of fluid intake having no effect on the concentration of the urine. There are several different types of DI, each with a different cause...
.
Cardiogenic
This type of shock is caused by the failure of the heart to pump effectively. This can be due to damage to the heart muscle, most often from a large myocardial infarctionMyocardial infarction
Myocardial infarction or acute myocardial infarction , commonly known as a heart attack, results from the interruption of blood supply to a part of the heart, causing heart cells to die...
. Other causes of cardiogenic shock include dysrhythmia
Cardiac dysrhythmia
Cardiac dysrhythmia is any of a large and heterogeneous group of conditions in which there is abnormal electrical activity in the heart. The heart beat may be too fast or too slow, and may be regular or irregular.Some arrhythmias are life-threatening medical emergencies that can result in cardiac...
s, cardiomyopathy
Cardiomyopathy
Cardiomyopathy, which literally means "heart muscle disease," is the deterioration of the function of the myocardium for any reason. People with cardiomyopathy are often at risk of arrhythmia or sudden cardiac death or both. Cardiomyopathy can often go undetected, making it especially dangerous to...
/myocarditis
Myocarditis
Myocarditis is inflammation of heart muscle . It resembles a heart attack but coronary arteries are not blocked.Myocarditis is most often due to infection by common viruses, such as parvovirus B19, less commonly non-viral pathogens such as Borrelia burgdorferi or Trypanosoma cruzi, or as a...
, congestive heart failure
Congestive heart failure
Heart failure often called congestive heart failure is generally defined as the inability of the heart to supply sufficient blood flow to meet the needs of the body. Heart failure can cause a number of symptoms including shortness of breath, leg swelling, and exercise intolerance. The condition...
(CHF), contusio cordis, or cardiac valveproblems.
Obstructive
Obstructive shock is due to obstruction of blood flow outside of the heart. Several conditions can result in this form of shock.- Cardiac tamponadeCardiac tamponadeCardiac tamponade, also known as pericardial tamponade, is an emergency condition in which fluid accumulates in the pericardium ....
in which fluid in the pericardium prevents inflow of blood into the heart (venous return). Constrictive pericarditisConstrictive pericarditisIn many cases, constrictive pericarditis is a late sequela, in other words a condition that is the consequence of a previous disease, of an inflammatory condition of the pericardium...
, in which the pericardiumPericardiumThe pericardium is a double-walled sac that contains the heart and the roots of the great vessels.-Layers:...
shrinks and hardens, is similar in presentation. - Tension pneumothorax Through increased intrathoracic pressure, bloodflow to the heart is prevented (venous return).
- Pulmonary embolismPulmonary embolismPulmonary embolism is a blockage of the main artery of the lung or one of its branches by a substance that has travelled from elsewhere in the body through the bloodstream . Usually this is due to embolism of a thrombus from the deep veins in the legs, a process termed venous thromboembolism...
is the result of a thromboembolic incident in the bloodvessels of the lungLungThe lung is the essential respiration organ in many air-breathing animals, including most tetrapods, a few fish and a few snails. In mammals and the more complex life forms, the two lungs are located near the backbone on either side of the heart...
s and hinders the return of blood to the heart. - Aortic stenosis hinders circulation by obstructing the ventricular outflow tractVentricular outflow tractA ventricular outflow tract is a portion of either the left ventricle or right ventricle of the heart through which blood passes in order to enter the great arteries....
Distributive
Distributive shock is due to impaired utilization of oxygen and thus production of energy by the cell. Examples of this form of shock are:- Septic shockSeptic shockSeptic shock is a medical emergency caused by decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis, though the microbe may be systemic or localized to a particular site. It can cause multiple organ dysfunction syndrome and death...
is the most common cause of distributive shock. Caused by an overwhelming systemic infection resulting in vasodilationVasodilationVasodilation refers to the widening of blood vessels resulting from relaxation of smooth muscle cells within the vessel walls, particularly in the large arteries, smaller arterioles and large veins. The process is essentially the opposite of vasoconstriction, or the narrowing of blood vessels. When...
leading to hypotension. Septic shock can be caused by Gram negative bacteria such as (among others) Escherichia coliEscherichia coliEscherichia coli is a Gram-negative, rod-shaped bacterium that is commonly found in the lower intestine of warm-blooded organisms . Most E. coli strains are harmless, but some serotypes can cause serious food poisoning in humans, and are occasionally responsible for product recalls...
, Proteus species, Klebsiella pneumoniaeKlebsiella pneumoniaeKlebsiella pneumoniae is a Gram-negative, non-motile, encapsulated, lactose fermenting, facultative anaerobic, rod shaped bacterium found in the normal flora of the mouth, skin, and intestines....
which release an endotoxinEndotoxinEndotoxins are toxins associated with some Gram-negative bacteria. An "endotoxin" is a toxin that is a structural molecule of the bacteria that is recognized by the immune system.-Gram negative:...
which produces adverse biochemical, immunological and occasionally neurological effects which are harmful to the body, and other Gram-positiveGram-positiveGram-positive bacteria are those that are stained dark blue or violet by Gram staining. This is in contrast to Gram-negative bacteria, which cannot retain the crystal violet stain, instead taking up the counterstain and appearing red or pink...
cocci, such as pneumococci and streptococci, and certain fungi as well as Gram-positive bacterial toxins. Septic shock also includes some elements of cardiogenic shock. In 1992, the ACCP/SCCM Consensus Conference Committee defined septic shock: ". . .sepsis-induced hypotension (systolic blood pressure <90 mm Hg or a reduction of 40 mm Hg from baseline) despite adequate fluid resuscitation along with the presence of perfusion abnormalities that may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. Patients who are receiving inotropic or vasopressor agents may have a normalized blood pressure at the time that perfusion abnormalities are identified." - Anaphylactic shock Caused by a severe anaphylactic reactionAnaphylaxisAnaphylaxis is defined as "a serious allergic reaction that is rapid in onset and may cause death". It typically results in a number of symptoms including throat swelling, an itchy rash, and low blood pressure...
to an allergenAllergenAn allergen is any substance that can cause an allergy. In technical terms, an allergen is a non-parasitic antigen capable of stimulating a type-I hypersensitivity reaction in atopic individuals....
, antigenAntigenAn antigen is a foreign molecule that, when introduced into the body, triggers the production of an antibody by the immune system. The immune system will then kill or neutralize the antigen that is recognized as a foreign and potentially harmful invader. These invaders can be molecules such as...
, drugDrugA drug, broadly speaking, is any substance that, when absorbed into the body of a living organism, alters normal bodily function. There is no single, precise definition, as there are different meanings in drug control law, government regulations, medicine, and colloquial usage.In pharmacology, a...
or foreign protein causing the release of histamineHistamineHistamine is an organic nitrogen compound involved in local immune responses as well as regulating physiological function in the gut and acting as a neurotransmitter. Histamine triggers the inflammatory response. As part of an immune response to foreign pathogens, histamine is produced by...
which causes widespread vasodilation, leading to hypotension and increased capillary permeability. - High spinal injuries may cause neurogenic shockNeurogenic shockNeurogenic shock is a distributive type of shock resulting in hypotension, occasionally with bradycardia, that is attributed to the disruption of the autonomic pathways within the spinal cord. Hypotension occurs due to decreased systemic vascular resistance resulting in pooling of blood within the...
. The classic symptoms include a slow heartrateBradycardiaBradycardia , in the context of adult medicine, is the resting heart rate of under 60 beats per minute, though it is seldom symptomatic until the rate drops below 50 beat/min. It may cause cardiac arrest in some patients, because those with bradycardia may not be pumping enough oxygen to their heart...
due to loss of cardiac sympathetic toneSympathetic nervous systemThe sympathetic nervous system is one of the three parts of the autonomic nervous system, along with the enteric and parasympathetic systems. Its general action is to mobilize the body's nervous system fight-or-flight response...
and warm skin due to dilation of the peripheral blood vessels. (This term can be confused with spinal shockSpinal shockSpinal shock was first defined by Whytt in 1750 as a loss of sensation accompanied by motor paralysis with initial loss but gradual recovery of reflexes, following a spinal cord injury – most often a complete transection. Reflexes in the spinal cord caudal to the SCI are depressed or absent ,...
which is a recoverable loss of function of the spinal cordSpinal cordThe spinal cord is a long, thin, tubular bundle of nervous tissue and support cells that extends from the brain . The brain and spinal cord together make up the central nervous system...
after injury and does not refer to the haemodynamic instability per se.)
Endocrine
Based on endocrine disturbances such as:- HypothyroidismHypothyroidismHypothyroidism is a condition in which the thyroid gland does not make enough thyroid hormone.Iodine deficiency is the most common cause of hypothyroidism worldwide but it can be caused by other causes such as several conditions of the thyroid gland or, less commonly, the pituitary gland or...
(Can be considered a form of Cardiogenic shockCardiogenic shockCardiogenic shock is based upon an inadequate circulation of blood due to primary failure of the ventricles of the heart to function effectively....
) in critically ill patients, reduces cardiac outputCardiac outputCardiac output is the volume of blood being pumped by the heart, in particular by a left or right ventricle in the time interval of one minute. CO may be measured in many ways, for example dm3/min...
and can lead to hypotensionHypotensionIn physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
and respiratory insufficiency. - ThyrotoxicosisHyperthyroidismHyperthyroidism is the term for overactive tissue within the thyroid gland causing an overproduction of thyroid hormones . Hyperthyroidism is thus a cause of thyrotoxicosis, the clinical condition of increased thyroid hormones in the blood. Hyperthyroidism and thyrotoxicosis are not synonymous...
(Cardiogenic shockCardiogenic shockCardiogenic shock is based upon an inadequate circulation of blood due to primary failure of the ventricles of the heart to function effectively....
)- may induce a reversible cardiomyopathy.
- Acute adrenal insufficiencyAdrenal insufficiencyAdrenal insufficiency is a condition in which the adrenal glands, located above the kidneys, do not produce adequate amounts of steroid hormones , primarily cortisol, but may also include impaired aldosterone production which regulates sodium, potassium and water retention...
(Distributive shockDistributive shockDistributive shock is defined by hypotension and generalized tissular hypoxia. This form of relative hypovolemia is the result of blood vessel dilation...
) is frequently the result of discontinuing corticosteroidCorticosteroidCorticosteroids are a class of steroid hormones that are produced in the adrenal cortex. Corticosteroids are involved in a wide range of physiologic systems such as stress response, immune response and regulation of inflammation, carbohydrate metabolism, protein catabolism, blood electrolyte...
treatment without tapering the dosage. However, surgery and intercurrent disease in patients on corticosteroid therapy without adjusting the dosage to accommodate for increased requirements may also result in this condition. - Relative adrenal insufficiency (Distributive shockDistributive shockDistributive shock is defined by hypotension and generalized tissular hypoxia. This form of relative hypovolemia is the result of blood vessel dilation...
) in critically ill patients where present hormone levelsCortisolCortisol is a steroid hormone, more specifically a glucocorticoid, produced by the adrenal gland. It is released in response to stress and a low level of blood glucocorticoids. Its primary functions are to increase blood sugar through gluconeogenesis; suppress the immune system; and aid in fat,...
are insufficient to meet the higher demands
Management
The best evidence exists for the treatment of septic shockSeptic shock
Septic shock is a medical emergency caused by decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis, though the microbe may be systemic or localized to a particular site. It can cause multiple organ dysfunction syndrome and death...
in adults and as the pathophysiology appears similar in children and other types of shock treatment this has been extrapolated to these areas. Management may include securing the airway via intubation
Intubation
Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic or rubber tube into the trachea to maintain an open airway or to serve as a conduit through which to administer certain drugs...
to decrease the work of breathing, oxygen supplementation, intravenous fluids and a passive leg raise (not Trendelenburg position
Trendelenburg position
In the Trendelenburg position the body is laid flat on the back with the feet higher than the head by 15-30 degrees, in contrast to the reverse Trendelenburg position, where the body is tilted in the opposite direction. This is a standard position used in abdominal and gynecological surgery...
), and blood transfusions. It is important to keep the person warm as well as adequately manage pain and anxiety as these can increase oxygen consumption.
Fluids
Aggressive intravenous fluids are recommended in most types of shock (e.g. 1-2 liter normal saline bolus over 10 minutes or 20ml/kg in a child) which is usually instituted as the person is being further evaluated. Which intravenous fluid is superior, colloids or crystalloids, remains undetermined. Thus as crystalloids are less expensive they are recommended. If the person remains in shock after initial resuscitation packed red blood cellsPacked red blood cells
In transfusion medicine, packed red blood cells are red blood cells that have been separated from whole blood for transfusion purposes. The product is typically abbreviated RBC or PRBC, and sometimes LRBC for leukoreduced products...
should be administered to keep the hemoglobin
Hemoglobin
Hemoglobin is the iron-containing oxygen-transport metalloprotein in the red blood cells of all vertebrates, with the exception of the fish family Channichthyidae, as well as the tissues of some invertebrates...
greater than 100 gms/l.
For those with hemorrhagic shock the current evidence supports limiting the use of fluids for penetrating thorax and abdominal injuries allowing mild hypotension
Hypotension
In physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
to persist (known as permissive hypotension
Permissive hypotension
Permissive hypotension or hypotensive resuscitation is a term used to describe the use of restrictive fluid therapy, specifically in the trauma patient, that increases systemic pressure without reaching normotension...
). Targets include a mean arterial pressure
Mean arterial pressure
The mean arterial pressure is a term used in medicine to describe an average blood pressure in an individual. It is defined as the average arterial pressure during a single cardiac cycle.-Calculation:...
of 60 mmHg, a systolic blood pressure of 70-90 mmHg, or until their adequate mentation and peripheral pulses.
Medications
Vasopressors may be used if blood pressure does not improve with fluids. There is no evidence of superiority of one vasopressor over another. Vasopressors have not been found to improve outcomes when used for hemorrhagic shock from traumaTrauma
Trauma can refer to:-In psychology and medicine:* Trauma , an often serious and body-altering physical injury, such as the removal of a limb...
but may be of use in neurogenic shock
Neurogenic shock
Neurogenic shock is a distributive type of shock resulting in hypotension, occasionally with bradycardia, that is attributed to the disruption of the autonomic pathways within the spinal cord. Hypotension occurs due to decreased systemic vascular resistance resulting in pooling of blood within the...
. Activated protein C (Xigris) while once aggressively promoted for the management of septic shock
Septic shock
Septic shock is a medical emergency caused by decreased tissue perfusion and oxygen delivery as a result of severe infection and sepsis, though the microbe may be systemic or localized to a particular site. It can cause multiple organ dysfunction syndrome and death...
has not been found to improve survival and is associated with a number of complications, thus is no longer recommended. The use of sodium bicarbonate
Sodium bicarbonate
Sodium bicarbonate or sodium hydrogen carbonate is the chemical compound with the formula Na HCO3. Sodium bicarbonate is a white solid that is crystalline but often appears as a fine powder. It has a slightly salty, alkaline taste resembling that of washing soda . The natural mineral form is...
is controversial as it has not been shown to improve outcomes. If used at all it should only be considered if the pH is less than 7.0.
Treatment goals
The goal of treatment is to achieve a urine output of greater than 0.5 cc/kg/hr, a central venous pressureCentral venous pressure
Central venous pressure describes the pressure of blood in the thoracic vena cava, near the right atrium of the heart...
of 8-12 mmHg and a mean arterial pressure
Mean arterial pressure
The mean arterial pressure is a term used in medicine to describe an average blood pressure in an individual. It is defined as the average arterial pressure during a single cardiac cycle.-Calculation:...
of 65-95 mmHg. In trauma the goal is to stop the bleeding which in many cases requires surgical interventions.