
Basal cell carcinoma
Encyclopedia
Basal-cell carcinoma is the most common type of skin cancer
. It rarely metastasizes
or kills. However, because it can cause significant destruction and disfigurement by invading surrounding tissues, it is still considered malignant
. Statistically, approximately 3 out of 10 Caucasians
may develop a basal-cell cancer within their lifetime. In 80 percent of all cases, basal-cell cancers are found on the head and neck. There appears to be an increase in the incidence of basal-cell cancer of the trunk (torso) in recent years.
For simplicity, one can also divide basal-cell carcinoma into 3 groups, based on location and difficulty of therapy:
See also:
. Infiltrative or morpheaform basal-cell cancers can present as a skin thickening or scar
tissue – making diagnosis difficult without using tactile sensation and a skin biopsy
. It is often difficult to distinguish basal-cell cancer from acne
scar, actinic elastosis
, and recent cryo
destruction inflammation
.
-exposed areas of the body. One-third occur on areas of the body that are not exposed to sunlight
, emphasizing the genetic susceptibility of basal-cell cancer patients.
is taken for pathological study. The most common method is a shave biopsy under local anesthesia
. Most nodular basal-cell cancers can be diagnosed clinically; however, other variants can be very difficult to distinguish from benign lesions such as intradermal nevus, sebaceomas, fibrous papules, early acne scars, and hypertrophic scarring.
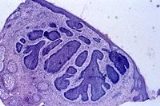
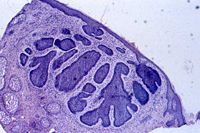 Basal-cell carcinomas develop in the basal cell layer of the skin
Basal-cell carcinomas develop in the basal cell layer of the skin
. Sun light exposure leads to the formation of thymine dimers, a form of DNA damage. While DNA repair
removes most UV-induced damage, not all crosslinks are excised. There is, therefore, cumulative DNA damage leading to mutation
s. Apart from the mutagenesis, sunlight depresses the local immune system
, possibly decreasing immune surveillance for new tumor cells.
Basal-cell carcinoma also develops as a result of Basal-Cell Nevus Syndrome, or Gorlin Syndrome, which is also characterized by keratocystic odontogenic tumors of the jaw, palmar or plantar (sole of the foot) pits, calcification of the falx cerebri
(in the center line of the brain) and rib abnormalities. The cause of the syndrome is a mutation in the PTCH1
tumor-suppressor gene at chromosome 9q22.3, which inhibits the hedgehog signaling pathway
. A mutation in the SMO
gene, which is also on the hedgehog pathway, also causes basal-cell carcinoma.
The use of a chemotherapeutic agent such as 5-Fluorouracil or Imiquimod
, can prevent development of skin cancer. It is usually recommended to individuals with extensive sun damage, history of multiple skin cancers, or precancerous growths. It is often repeated every 2 to 3 years to further decrease the risk of skin cancer.
Treating surgeons will recommend one of these modalities as appropriate treatment depending on the tumour size, location, patient age, and other variables.
, it grows locally with invasion and destruction of local tissues. The cancer can impinge on vital structures like nerves and result in loss of sensation or loss of function or rarely death
. The vast majority of cases can be successfully treated before serious complications occur. The recurrence rate for the above treatment options ranges from 50 percent to 1 percent or less.
alone. Up to 30% of caucasians develop basal-cell carcinomas in their lifetime. In Canada, the most common skin cancer is basal cell carcinoma (as much as one third of all cancer diagnoses), affecting 1 in 7 individuals over a lifetime.
Most sporadic BCC arises in small numbers on sun-exposed skin of people over age 50, although younger people may also be affected. The development of multiple basal-cell cancer at an early age could be indicative of Nevoid basal-cell carcinoma syndrome.
Skin cancer
Skin neoplasms are skin growths with differing causes and varying degrees of malignancy. The three most common malignant skin cancers are basal cell cancer, squamous cell cancer, and melanoma, each of which is named after the type of skin cell from which it arises...
. It rarely metastasizes
Metastasis
Metastasis, or metastatic disease , is the spread of a disease from one organ or part to another non-adjacent organ or part. It was previously thought that only malignant tumor cells and infections have the capacity to metastasize; however, this is being reconsidered due to new research...
or kills. However, because it can cause significant destruction and disfigurement by invading surrounding tissues, it is still considered malignant
Malignant
Malignancy is the tendency of a medical condition, especially tumors, to become progressively worse and to potentially result in death. Malignancy in cancers is characterized by anaplasia, invasiveness, and metastasis...
. Statistically, approximately 3 out of 10 Caucasians
White people
White people is a term which usually refers to human beings characterized, at least in part, by the light pigmentation of their skin...
may develop a basal-cell cancer within their lifetime. In 80 percent of all cases, basal-cell cancers are found on the head and neck. There appears to be an increase in the incidence of basal-cell cancer of the trunk (torso) in recent years.
Classification
Basal-cell carcinomas may be divided into the following types:- Nodular basal-cell carcinoma (Classic basal-cell carcinoma)
- Cystic basal-cell carcinoma
- Cicatricial basal-cell carcinoma (Morpheaform basal-cell carcinoma, Morphoeic basal-cell carcinoma)
- Infiltrative basal-cell carcinoma
- Micronodular basal-cell carcinoma
- Superficial basal-cell carcinoma (Superficial multicentric basal-cell carcinoma)
- Pigmented basal-cell carcinoma
- Rodent ulcerRodent ulcerRodent ulcer is a large skin lesion of nodular basal cell carcinoma with central necrosis. and is type of Basal cell carcinoma...
(Jacobi ulcer) - Fibroepithelioma of PinkusFibroepithelioma of PinkusFibroepithelioma of Pinkus is a cutaneous condition, a subtype of basal cell carcinoma, most commonly occurring on the lower back....
- Polypoid basal-cell carcinoma
- Pore-like basal-cell carcinoma
- Aberrant basal-cell carcinoma
For simplicity, one can also divide basal-cell carcinoma into 3 groups, based on location and difficulty of therapy:
- Superficial basal-cell carcinoma, or some might consider to be equivalent to "in-situ". Very responsive to topical chemotherapy such as AldaraImiquimodImiquimod is a prescription medication that acts as an immune response modifier. It is marketed by Meda AB, Graceway Pharmaceuticals and iNova Pharmaceuticals under the trade names Aldara and Zyclara, and by Mochida as Beselna. It is also referred to as R-837.- History :The original FDA approval...
, or FluorouracilFluorouracilFluorouracil is a drug that is a pyrimidine analog which is used in the treatment of cancer. It is a suicide inhibitor and works through irreversible inhibition of thymidylate synthase. It belongs to the family of drugs called antimetabolites...
. It is the only type of basal-cell cancer that can be effectively treated with topical chemotherapy. - Infiltrative basal-cell carcinoma, which often encompasses morpheaform and micronodular basal-cell cancer. More difficult to treat with conservative treatment methods such as electrodessiccation and currettage, or with currettage alone.
- Nodular basal-cell carcinoma, which essentially includes most of the remaining categories of basal-cell cancer. It is not unusual to encounter morphologic features of several variants of basal-cell cancer in the same tumor.
See also:
- Nevoid basal-cell carcinoma syndrome
Signs and symptoms
Patients present with a shiny, pearly nodule. However, superficial basal-cell cancer can present as a red patch like eczemaEczema
Eczema is a form of dermatitis, or inflammation of the epidermis . In England, an estimated 5.7 million or about one in every nine people have been diagnosed with the disease by a clinician at some point in their lives.The term eczema is broadly applied to a range of persistent skin conditions...
. Infiltrative or morpheaform basal-cell cancers can present as a skin thickening or scar
Scar
Scars are areas of fibrous tissue that replace normal skin after injury. A scar results from the biological process of wound repair in the skin and other tissues of the body. Thus, scarring is a natural part of the healing process. With the exception of very minor lesions, every wound results in...
tissue – making diagnosis difficult without using tactile sensation and a skin biopsy
Biopsy
A biopsy is a medical test involving sampling of cells or tissues for examination. It is the medical removal of tissue from a living subject to determine the presence or extent of a disease. The tissue is generally examined under a microscope by a pathologist, and can also be analyzed chemically...
. It is often difficult to distinguish basal-cell cancer from acne
Acne
Acne is a general term used for acneiform eruptions. It is usually used as a synonym for acne vulgaris, but may also refer to:*Acne aestivalis*Acne conglobata*Acne cosmetica*Acne fulminans*Acne keloidalis nuchae*Acne mechanica...
scar, actinic elastosis
Actinic elastosis
Actinic, or solar, elastosis is an accumulation of abnormal elastin in the dermis of the skin, and in the conjunctiva of the eye, which occurs as a result of the cumulative effects of prolonged and excessive sun exposure, a process known as photoaging.-Clinical features:Actinic elastosis usually...
, and recent cryo
Cryo
The word cryo or cryos is Greek and means "icy cold" . The word is also known from cryobiology. Cryos or Cryos International is also an international network of sperm banks...
destruction inflammation
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
.
Distribution
About two thirds of basal-cell carcinomas occur on sunSun
The Sun is the star at the center of the Solar System. It is almost perfectly spherical and consists of hot plasma interwoven with magnetic fields...
-exposed areas of the body. One-third occur on areas of the body that are not exposed to sunlight
Sunlight
Sunlight, in the broad sense, is the total frequency spectrum of electromagnetic radiation given off by the Sun. On Earth, sunlight is filtered through the Earth's atmosphere, and solar radiation is obvious as daylight when the Sun is above the horizon.When the direct solar radiation is not blocked...
, emphasizing the genetic susceptibility of basal-cell cancer patients.
Diagnosis
To diagnose basal-cell carcinomas, a skin biopsySkin biopsy
Skin biopsy is a biopsy technique in which a skin lesion is removed and sent to the pathologist to render a microscopic diagnosis. It is usually done under local anesthetic in a physician's office, and results are often available in 4 to 10 days. It is commonly performed by dermatologists. Skin...
is taken for pathological study. The most common method is a shave biopsy under local anesthesia
Anesthesia
Anesthesia, or anaesthesia , traditionally meant the condition of having sensation blocked or temporarily taken away...
. Most nodular basal-cell cancers can be diagnosed clinically; however, other variants can be very difficult to distinguish from benign lesions such as intradermal nevus, sebaceomas, fibrous papules, early acne scars, and hypertrophic scarring.
Pathophysiology
Skin
-Dermis:The dermis is the layer of skin beneath the epidermis that consists of connective tissue and cushions the body from stress and strain. The dermis is tightly connected to the epidermis by a basement membrane. It also harbors many Mechanoreceptors that provide the sense of touch and heat...
. Sun light exposure leads to the formation of thymine dimers, a form of DNA damage. While DNA repair
DNA repair
DNA repair refers to a collection of processes by which a cell identifies and corrects damage to the DNA molecules that encode its genome. In human cells, both normal metabolic activities and environmental factors such as UV light and radiation can cause DNA damage, resulting in as many as 1...
removes most UV-induced damage, not all crosslinks are excised. There is, therefore, cumulative DNA damage leading to mutation
Mutation
In molecular biology and genetics, mutations are changes in a genomic sequence: the DNA sequence of a cell's genome or the DNA or RNA sequence of a virus. They can be defined as sudden and spontaneous changes in the cell. Mutations are caused by radiation, viruses, transposons and mutagenic...
s. Apart from the mutagenesis, sunlight depresses the local immune system
Immune system
An immune system is a system of biological structures and processes within an organism that protects against disease by identifying and killing pathogens and tumor cells. It detects a wide variety of agents, from viruses to parasitic worms, and needs to distinguish them from the organism's own...
, possibly decreasing immune surveillance for new tumor cells.
Basal-cell carcinoma also develops as a result of Basal-Cell Nevus Syndrome, or Gorlin Syndrome, which is also characterized by keratocystic odontogenic tumors of the jaw, palmar or plantar (sole of the foot) pits, calcification of the falx cerebri
Falx cerebri
The falx cerebri, also known as the cerebral falx, so named from its sickle-like form, is a strong, arched fold of dura mater which descends vertically in the longitudinal fissure between the cerebral hemispheres....
(in the center line of the brain) and rib abnormalities. The cause of the syndrome is a mutation in the PTCH1
PTCH1
Protein patched homolog 1 is a protein that is the member of the Patched family and in humans is encoded by the PTCH1 gene.- Function :PTCH1 is a member of the patched gene family and is the receptor for sonic hedgehog, a secreted molecule implicated in the formation of embryonic structures and in...
tumor-suppressor gene at chromosome 9q22.3, which inhibits the hedgehog signaling pathway
Hedgehog signaling pathway
In a growing embryo, cells develop differently in the head or tail end of the embryo, the left or right, and other positions. They also form segments which develop into different body parts. The hedgehog signaling pathway gives cells information that they need to make the embryo develop properly....
. A mutation in the SMO
Smoothened
Smoothened is a G protein-coupled receptor protein encoded by the gene of the hedgehog pathway conserved from flies to humans. It is the molecular target of the teratogen cyclopamine....
gene, which is also on the hedgehog pathway, also causes basal-cell carcinoma.
Prevention
Basal-cell carcinoma is the most common skin cancer. It occurs mainly in fair-skinned patients with a family history of this cancer. Sunlight is a factor in about two-thirds of these cancers; therefore, doctors recommend sun screens with at least SPF 30. One-third occur in non-sun-exposed areas.The use of a chemotherapeutic agent such as 5-Fluorouracil or Imiquimod
Imiquimod
Imiquimod is a prescription medication that acts as an immune response modifier. It is marketed by Meda AB, Graceway Pharmaceuticals and iNova Pharmaceuticals under the trade names Aldara and Zyclara, and by Mochida as Beselna. It is also referred to as R-837.- History :The original FDA approval...
, can prevent development of skin cancer. It is usually recommended to individuals with extensive sun damage, history of multiple skin cancers, or precancerous growths. It is often repeated every 2 to 3 years to further decrease the risk of skin cancer.
Treatment
The following methods are employed in the treatment of basal-cell carcinoma (BCC):- Standard surgical excision with either frozen section histologyHistologyHistology is the study of the microscopic anatomy of cells and tissues of plants and animals. It is performed by examining cells and tissues commonly by sectioning and staining; followed by examination under a light microscope or electron microscope...
, or paraffin embedded fixed tissue pathology. This is the preferred method for removal of most BCCs. The cure rate for this method, whether done by a plastic surgeon, family doctor, or dermatologist is totally dependent on the surgical marginSurgical marginSurgical margin, also known as tumor free margin, free margin, normal skin margin, and normal tissue margin, usually refers to the visible normal tissue or skin margin that is removed with the surgical excision of a tumor, growth, or malignancy.-Definition:Surgical margin in a surgery reports...
. When standard surgical margin is applied (usually 4 mm or more), a high cure rate can be achieved with standard excision A dermatoscope can help an experienced surgeon accurately identify the visible tumour that the naked eye can not see. The narrower the free surgical margin (skin removed that is free of visible tumor) the higher the recurrence rate. A weakness with standard surgical excision is the high recurrence rate of basal-cell cancers of the face, especially around eyelids, nose, and facial structures. A diagram on page 33 of the NCCN publication demonstrate the area of high risk of recurrence as most the face with the exception of the central cheek and upper forehead. On the face, or on recurrent basal-cell cancer after previous surgery, special surgical margin controlled processing (CCPDMACCPDMACCPDMA is the acronym for "complete circumferential peripheral and deep margin assessment". It is the preferred method for the removal of certain cancers, especially skin cancers.A classical example of CCPDMA is Mohs surgery...
- complete circumferential peripheral and deep margin assessment) using frozen section histology (Mohs surgeryMohs surgeryMohs surgery, also known as chemosurgery, created by a general surgeon, Dr. Frederic E. Mohs, is microscopically controlled surgery used to treat common types of skin cancer. It is one of the many methods of obtaining complete margin control during removal of a skin cancer using frozen section...
is one of the methods) is required. With surgical margin controlled frozen section histology, a surgeon can achieve a high cure rate and low recurrence rate on the same day of the excision. However, most standard excisions done in a plastic surgeon or dermatologist's office are sent to an outside laboratory for standard bread loafingBread loafingBread loafing is a common method of processing surgical specimen for histopathology. The process involves cutting the specimen into 3 or more sections. The cut sections are mounted by embedding in paraffin or frozen medium. The cut edge is then thinly sliced with a microtome or a cryostat...
method of processing. This method has a high "false negative" rate due to the random sampling of the tumour. It is likely that less than 5% of the surgical margin is examined, as each slice of tissue is only 6 micrometres thick, about 3 to 4 serial slices are obtained per section, and only about 3 to 4 sections are obtained per specimen (see figure 2 of reference). Usually, the rule of thumb is if a 4 mm free surgical margin is obtained around a small tumor (less than 6mm), or a wider 6 mm free surgical margin is obtained around a larger tumor (greater than 6mm), the cure rate is very high - 95% or better. For cosmetic reasons, many doctors take only very small surgical margins 1–2 mm, especially when facial tumour is being removed. A pathology report from such a case indicating "margins free of residual tumour", often is inaccurate, and a high recurrence rate of up to 38% might occur. When in doubt, a patient should demand that either Mohs surgery or frozen section histology with either margin control (ccpdma) or thin serial bread-loafing is utilized when dealing with a tumour on the face. The pathologist processing the frozen section specimen should cut multiple sections through the block to minimize the false negative error rate. Or one should simply process the tissue utilizing a method approximating the Mohs method (described in most basic histopathology text books or described in this reference ) during frozen section processing. Unfortunately, these methods are difficult when applied to frozen sections; and is very tedious to process. When not utilizing frozen section, the surgeon might have to wait a week or more, before informing the patient if more tumour is left, or if the surgical margin is too narrow. And a second surgery must be performed to remove the residual or potential residual tumour once the surgeon inform the patient of the positive or narrow surgical margin on the surgical pathology report.
- Mohs surgery: Mohs surgeryMohs surgeryMohs surgery, also known as chemosurgery, created by a general surgeon, Dr. Frederic E. Mohs, is microscopically controlled surgery used to treat common types of skin cancer. It is one of the many methods of obtaining complete margin control during removal of a skin cancer using frozen section...
(or Mohs micrographic surgery) is an outpatient procedure in which the tumor is surgically excised and then immediately examined under a microscope. It is a form of pathology processing called CCPDMACCPDMACCPDMA is the acronym for "complete circumferential peripheral and deep margin assessment". It is the preferred method for the removal of certain cancers, especially skin cancers.A classical example of CCPDMA is Mohs surgery...
. It is claimed to have the highest cure rate of 97% to 99.8% by some individuals. The base and edges are microscopically examined to verify sufficient margins before the surgical repair of the site. If the margins are insufficient, more is removed from the patient until the margins are sufficient. It is also used for squamous-cell carcinoma; however, the cure rate is not as high as Mohs surgery for basal-cell carcinoma.
- Chemotherapy: Some superficial cancers respond to local therapy with 5-fluorouracil, a chemotherapyChemotherapyChemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
agent. Topical treatment with 5% ImiquimodImiquimodImiquimod is a prescription medication that acts as an immune response modifier. It is marketed by Meda AB, Graceway Pharmaceuticals and iNova Pharmaceuticals under the trade names Aldara and Zyclara, and by Mochida as Beselna. It is also referred to as R-837.- History :The original FDA approval...
cream, with five applications per week for six weeks has a reported 70-90% success rate at reducing, even removing, the BCC [basal-cell carcinoma]. Both Imiquimod and 5-fluorouracil have received FDA approval for the treatment of superficial basal-cell carcinoma. Off label use of imiquimod on invasive basal-cell carcinoma has been reported. Imiquimod may be used prior to surgery in order to reduce the size of the carcinoma. One can expect a great deal of inflammation with this treatment. Chemotherapy often follows Mohs surgery to eliminate the residual superficial basal-cell carcinoma after the invasive portion is removed. Some advocate the use of imiquimod prior to Mohs surgery to remove the superficial component of the cancer Removing the residual superficial tumor with surgery alone can result in large and difficult to repair surgical defects. One often waits a month or more after surgery before starting the Imiquimod or 5-fluorouracil to make sure the surgical wound has adequately healed. Some individuals advocate the use of curettage (see EDC below) first, then followed by chemotherapy. These experimental procedure likely will result in better cure rate than one alone, but are not standard care.
- Immunotherapy: ImmunotherapyImmunotherapyImmunotherapy is a medical term defined as the "treatment of disease by inducing, enhancing, or suppressing an immune response". Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies. While immunotherapies that reduce or suppress are...
research suggests that treatment using Euphorbia peplusEuphorbia peplusEuphorbia peplus is a species of Euphorbia, native to most of Europe, northern Africa, and western Asia, where it typically grows in cultivated arable land, gardens, and other disturbed land.Outside of its native range it is very widely naturalised and often invasive, including in Australia, New...
, a common garden weed, may be effective. Australian biopharmaceutical company Peplin is developing this as topical treatment for BCC. ImiquimodImiquimodImiquimod is a prescription medication that acts as an immune response modifier. It is marketed by Meda AB, Graceway Pharmaceuticals and iNova Pharmaceuticals under the trade names Aldara and Zyclara, and by Mochida as Beselna. It is also referred to as R-837.- History :The original FDA approval...
or Aldara is an immunotherapy but is listed here under chemotherapy.
- Radiation: Radiation therapyRadiation therapyRadiation therapy , radiation oncology, or radiotherapy , sometimes abbreviated to XRT or DXT, is the medical use of ionizing radiation, generally as part of cancer treatment to control malignant cells.Radiation therapy is commonly applied to the cancerous tumor because of its ability to control...
is appropriate for all forms of BCC as adequate doses will eradicate the disease. Radiation therapy can be delivered either as external beam radiotherapyExternal beam radiotherapyExternal beam radiotherapy or teletherapy is the most common form of radiotherapy. The patient sits or lies on a couch and an external source of radiation is pointed at a particular part of the body...
or as brachytherapyBrachytherapyBrachytherapy , also known as internal radiotherapy, sealed source radiotherapy, curietherapy or endocurietherapy, is a form of radiotherapy where a radiation source is placed inside or next to the area requiring treatment...
(internal radiotherapy). Although radiotherapy is generally used in older patients who are not candidates for surgery, it is also used in cases where surgical excision will be disfiguring or difficult to reconstruct (especially on the tip of the nose, and the nostril rims). Radiation treatment often takes as few as 5 visits to as many as 25 visits for radiation therapy. Usually, the more visits scheduled for therapy, the less complication or damage is done to the normal tissue supporting the tumor. Radiotherapy can also be useful if surgical excision has been done incompletely or if the pathology report following surgery suggests a high risk of recurrence, for example if nerve involvement has been demonstrated. Cure rate can be as high as 95% for small tumor, or as low as 80% for large tumors. Usually, recurrent tumors after radiation are treated with surgery, and not with radiation. Further radiation treatment will further damage normal tissue, and the tumor might be resistant to further radiation.
- Photodynamic therapy: Photodynamic therapyPhotodynamic therapyPhotodynamic therapy is used clinically to treat a wide range of medical conditions, including malignant cancers, and is recognised as a treatment strategy which is both minimally invasive and minimally toxic...
is a new modality for treatment of basal-cell carcinoma, which is administrated by application of photosensitizers to the target area. When these molecules are activated by light, they become toxic, therefore destroy the target cells. Methyl aminolevulinateMethyl aminolevulinateMethyl aminolevulinate is a prodrug that is metabolised to Protoporphyrin IX used in photodynamic therapy. It is marketed as Metvix....
is approved by EU as a photosensitizer since 2001. This therapy is also used in other skin cancer types.
- Cryosurgery: CryosurgeryCryosurgeryCryosurgery is the application of extreme cold to destroy abnormal or diseased tissue. The term comes from the Greek words cryo and surgery meaning "hand work" or "handiwork"....
is an old modality for the treatment of many skin cancers. When accurately utilized with a temperature probe and cryotherapy instruments, it can result in very good cure rate. Disadvantages include lack of margin control, tissue necrosis, over or under treatment of the tumor, and long recovery time. Overall, there are sufficient data to consider cryosurgery as a reasonable treatment for BCC. There are no good studies, however, comparing cryosurgery with other modalities, particularly with Mohs surgery, excision, or electrodesiccation and curretage so that no conclusion can be made whether cryosurgery is as efficacious as other methods. Also, there is no evidence on whether curetting the lesions before cryosurgery affects the efficacy of treatment. Several textbooks are published on the therapy, and a few physicians still apply the treatment to selected patients.
- Electrodesiccation and curettage: or EDC is accomplished by using a round knife, or curette, to scrape away the soft cancer. The skin is then burned with an electric current. This further softens the skin, allowing for the knife to cut more deeply with the next layer of curettage. The cycle is repeated, with a safety margin of curettage of normal skin around the visible tumor. This cycle is repeated 3 to 5 times, and the free skin margin treated is usually 4 to 6 mm. Cure rate is very much user dependent and depends on the size and type of tumor. Infiltrative or morpheaform BCCs can be difficult to eradicate with EDC. Generally, this method is used on cosmetically unimportant areas like the trunk (torso). Some physicians believe that it is acceptable to utilize EDC on the face of elderly patients over the age of 70. However, with increasing life expectancy, such an objective criterion cannot be supported. The cure rate can be low or high, depending on the aggressiveness of the EDC and the free margin treated. Some advocate curettage alone without electrodesiccation, and with the same cure rate.
Treating surgeons will recommend one of these modalities as appropriate treatment depending on the tumour size, location, patient age, and other variables.
Prognosis
Prognosis is excellent if the appropriate method of treatment is used in early primary basal-cell cancers. Recurrent cancers are much harder to cure, with a higher recurrent rate with any methods of treatment. Although basal-cell carcinoma rarely metastasizesMetastasis
Metastasis, or metastatic disease , is the spread of a disease from one organ or part to another non-adjacent organ or part. It was previously thought that only malignant tumor cells and infections have the capacity to metastasize; however, this is being reconsidered due to new research...
, it grows locally with invasion and destruction of local tissues. The cancer can impinge on vital structures like nerves and result in loss of sensation or loss of function or rarely death
Death
Death is the permanent termination of the biological functions that sustain a living organism. Phenomena which commonly bring about death include old age, predation, malnutrition, disease, and accidents or trauma resulting in terminal injury....
. The vast majority of cases can be successfully treated before serious complications occur. The recurrence rate for the above treatment options ranges from 50 percent to 1 percent or less.
Epidemiology
Basal-cell cancer is the most common skin cancer. It is much more common in fair-skinned individuals with a family history of basal-cell cancer and increases in incidence closer to the equator or at higher altitude. According to Skin Cancer Foundation, there are approximately 800,000 new cases yearly in the United StatesUnited States
The United States of America is a federal constitutional republic comprising fifty states and a federal district...
alone. Up to 30% of caucasians develop basal-cell carcinomas in their lifetime. In Canada, the most common skin cancer is basal cell carcinoma (as much as one third of all cancer diagnoses), affecting 1 in 7 individuals over a lifetime.
Most sporadic BCC arises in small numbers on sun-exposed skin of people over age 50, although younger people may also be affected. The development of multiple basal-cell cancer at an early age could be indicative of Nevoid basal-cell carcinoma syndrome.