
Renal cell carcinoma
Encyclopedia
Renal cell carcinoma (RCC, also known as hypernephroma) is a kidney cancer
that originates in the lining of the proximal convoluted tubule
, the very small tubes in the kidney that filter the blood and remove waste products. RCC is the most common type of kidney cancer in adults, responsible for approximately 80% of cases. It is also known to be the most lethal of all the genitourinary tumors. Initial treatment is most commonly a radical or partial nephrectomy
and remains the mainstay of curative treatment. Where the tumor is confined to the renal parenchyma, the 5-year survival rate is 60-70%, but this is lowered considerably where metastases have spread. It is resistant to radiation therapy
and chemotherapy
, although some cases respond to immunotherapy
. Targeted cancer therapies such as sunitinib
, temsirolimus
, bevacizumab
, interferon-alpha, and possibly sorafenib
have improved the outlook for RCC (progression-free survival), although they have not yet demonstrated improved survival.
(blood in the urine), flank pain and an abdominal mass. This triad only occurs in 10-15% of cases, and is generally indicative of more advanced disease. Today, the majority of renal tumors are asymptomatic and are detected incidentally on imaging, usually for an unrelated cause.
Signs may include:
Patients may also experience the following symptoms:
_nephrectomy.jpg)

 Recent genetic studies have altered the approaches used in classifying renal cell carcinoma. The following system can be used to classify these tumors:
Recent genetic studies have altered the approaches used in classifying renal cell carcinoma. The following system can be used to classify these tumors:
Renal epithelial neoplasms have characteristic cytogenetic aberrations that can aid in classification. See also Atlas of Genetics and Cytogenetics in Oncology and Haematology.
Array-based karyotyping can be used to identify characteristic chromosomal aberrations in renal tumors with challenging morphology. Array-based karyotyping performs well on paraffin embedded tumors and is amenable to routine clinical use. See also Virtual Karyotype
for CLIA certified laboratories offering array-based karyotyping of solid tumors.
Other associated genes include TRC8, OGG1, HNF1A
, HNF1B
, TFE3
, RCCP3, and RCC17.
In Europe the incidence of RCC has doubled in the period from 1975 to 2005. RCC accounted for 3777 deaths in the UK in 2006; male 2372, female 1820.
. Hypertension
and a family history of the disease are also risk factors. Occupational exposure to cadmium is a risk factor.
Dialysis
patients with acquired cystic disease of the kidney showed a 30 times greater risk than in the general population for developing RCC.
Exposure to asbestos, polycyclic aromatic hydrocarbons, gasoline has not been shown to be consistently associated with RCC risk.
Patients with certain inherited disorders such as von Hippel-Lindau disease
, hereditary papillary renal cancer, a hereditary leiomyoma RCC syndrome and Birt-Hogg-Dubé syndrome, show an enhanced risk of RCC. Also, patients with sickle cell trait
are predisposed to developing Renal medullary carcinoma
.
Hysterectomy
is associated with an approximately doubled risk. Hormonal factors or injury of the ureter during surgery were considered as possible causes.
The first steps taken in order to diagnose this condition are observing any of the signs and symptoms, and an anamnesis
(the detailed medical review of past health state) to evaluate any risk factors. Upon physical examination
, palpation of the abdomen may reveal the presence of a mass or an organ enlargement.
However, the main diagnostic tool for detecting renal cell carcinoma is ultrasound
of the kidneys. If the ultrasound shows a mass or cyst, a subsequent abdominal CT is the optimal test for diagnosis and staging
.
Renal cell carcinoma may also be cystic. As there are several benign cystic renal lesions (simple renal cyst, hemorrhagic renal cyst, multilocular cystic nephroma, polycystic kidney disease), it may occasionally be difficult for the radiologist to differentiate a benign cystic lesion from a malignant one. A classification system for cystic renal lesions that classifies them based specific imaging features into groups that are benign and those that need surgical resection is available.
Percutaneous biopsy can be performed by a radiologist using ultrasound
or computed tomography
to guide sampling of the tumor for the purpose of diagnosis by pathology. However this is not routinely performed because when the typical imaging features of renal cell carcinoma are present, the possibility of an incorrectly negative result together with the risk of a medical complication to the patient make it unfavorable from a risk-benefit perspective. This is not completely accurate, there are new experimental treatments.
of renal cell carcinoma is the most important factor in predicting its prognosis. Staging can follow the TNM staging system, where the size and extent of the tumour (T), involvement of lymph nodes (N) and metastases (M) are classified separately. Also, it can use overall stage grouping into stage I-IV, with the 1997 revision of AJCC described below:
At diagnosis, 30% of renal cell carcinomas have spread to the ipsilateral renal vein, and 5-10% have continued into the inferior vena cava.
 The gross and microscopic appearance of renal cell carcinomas is highly variable. The following describes a typical clear cell carcinoma, which is the most common type.
The gross and microscopic appearance of renal cell carcinomas is highly variable. The following describes a typical clear cell carcinoma, which is the most common type.
The renal cell carcinoma may present reddened areas where blood vessels have bled, and cysts containing watery fluids. The body of the tumor shows large blood vessels that have walls composed of cancerous cells.
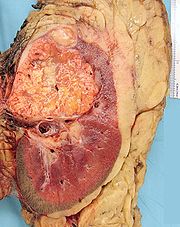
Gross examination
often shows a yellowish, multilobulated tumor in the renal cortex, which frequently contains zones of necrosis, hemorrhage and scarring.
Light microscopy shows tumor cells forming cords, papillae, tubules or nests, and are atypical, polygonal and large. Also, the cells that make up a renal carcinoma may be clear, granular, mixed clear and granular or sarcomatoid or spindle type. Recent studies have brought to attention that the type of cancerous cells and the aggressiveness of the condition are closely related.Because these cells accumulate glycogen
and lipid
s, their cytoplasm appear "clear", the nuclei remain in the middle of the cells, and the cellular membrane is evident. Some cells may be smaller, with eosinophilic cytoplasm, resembling normal tubular cells. The stroma is reduced, but well vascularized. The tumor compresses the surrounding parenchyma, producing a pseudocapsule.
The clear cells are thought to be the least likely to spread and usually respond more favorably to treatment. However, most of the tumors contain a mixture of cells. The most aggressive stage of renal cancer is believed to be the one in which the tumor is mixed, containing both clear and granular cells.
that used the 1997 AJCC staging system estimated the five year survival rate to be 90% for stage I, 51% for stage II, 22% for stage III and 4.6% for stage IV. The same study estimated the median survival time to be 7.7 years for stage I, 5.0 years for stage II, 3.1 years for stage III and 1.1 years for stage IV.
For those that have tumor recurrence after surgery, the prognosis is generally poor. Renal cell carcinoma does not generally respond to chemotherapy or radiation. Immunotherapy, which attempts to induce the body to attack the remaining cancer cells, has shown promise. Recent trials are testing newer agents, though the current complete remission rate with these approaches are still low, around 12-20% in most series. Most recently, treatment with tyrosine kinase inhibitors including nexavar, pazopanib
, and rapamycin have shown promise in improving the prognosis for advanced RCC since 2004.
. If it has spread outside of the kidneys, often into the lymph nodes or the main vein of the kidney, then it must be treated with adjunctive therapy, including cytoreductive surgery. RCC is resistant to chemotherapy and radiotherapy in most cases, but does respond well to immunotherapy with interleukin-2 or interferon-alpha, biologic, or targeted therapy. In early stage cases, cryotherapy and surgery are the preferred options.
when possible. Most of these small renal masses manifest indolent biological behavior with excellent prognosis. More centers of excellence are incorporating needle biopsy to confirm the presence of malignant histology prior to recommending definitive surgical extirpation. In the elderly, patients with co-morbidities and in poor surgical candidates, small renal tumors may be monitored carefully with serial imaging. Most clinicians conservatively follow tumors up to a size threshold between 3 and 5 cm, beyond which the risk of distant spread (metastases) is about 5%.
The most common application of cryoablation is to ablate solid tumors found in the lung, liver, breast, kidney and prostate. The use in prostate and renal cryoablation are the most common. Although sometimes applied through laparoscopic or open surgical approaches, most often cryoablation is performed percutaneously (through the skin and into the target tissue containing the tumor).
 Surgical removal of all or part of the kidney (nephrectomy
Surgical removal of all or part of the kidney (nephrectomy
) is recommended. This may include removal of the adrenal gland, retroperitoneal lymph nodes, and possibly tissues involved by direct extension (invasion) of the tumor into the surrounding tissues. In cases where the tumor has spread into the renal vein, inferior vena cava, and possibly the right atrium, this portion of the tumor can be surgically removed, as well. In cases of known metastases, surgical resection of the kidney ("cytoreductive nephrectomy") may improve survival, as well as resection of a solitary metastatic lesion. Kidneys are sometimes embolized
prior to surgery to minimize blood loss (see image).
Surgery is increasingly performed via laparoscopic
techniques. These have the advantage of being less of a burden for the patient and the disease-free survival is comparable to that of open surgery. For small exophytic lesions that do not extensively involve the major vessels or urinary collecting system, a partial nephrectomy (also referred to as "nephron sparing surgery") can be performed. This may involve temporarily stopping blood flow to the kidney while the mass is removed as well as renal cooling with an ice slush. Mannitol
can also be administered to help limit damage to the kidney. This is usually done through an open incision although smaller lesions can be done laparoscopically with or without robotic assistance.
Laparoscopic cryotherapy
can also be done on smaller lesions. Typically a biopsy is taken at the time of treatment. Intraoperative ultrasound may be used to help guide placement of the freezing probes. Two freeze/thaw cycles are then performed to kill the tumor cells. As the tumor is not removed followup is more complicated (see below) and overall disease free rates are not as good as those obtained with surgical removal.
, image-guided therapies, usually managed by radiologists, are being offered to patients with localized tumor, but who are not good candidates for a surgical procedure. This sort of procedure involves placing a probe through the skin and into the tumor using real-time imaging of both the probe tip and the tumor by computed tomography
, ultrasound
, or even magnetic resonance imaging
guidance, and then destroying the tumor with heat (radiofrequency ablation
) or cold (cryotherapy
). These modalities are at a disadvantage compared to traditional surgery in that pathologic confirmation of complete tumor destruction is not possible. Therefore, long-term follow-up is crucial to assess completeness of tumour ablation.
, an antibody to VEGF
, has significantly prolonged time to progression, but phase 3 trials have not been published. Sunitinib (Sutent), sorafenib (Nexavar), and temsirolimus, which are small-molecule inhibitors of proteins, have been approved by the U.S. F.D.A.
Treatment with tyrosine kinase inhibitors including Nexavar, pazopanib
, and rapamycin have shown promise in improving the prognosis for advanced RCC since 2004.
Sorafenib
(Nexavar), a protein kinase inhibitor, was FDA approved in December 2005 for treatment of advanced renal cell cancer.
A month later, Sunitinib
(Sutent) was approved as well. Sunitinib (an oral, small-molecule, multi-targeted (RTK) inhibitor) and sorafenib both interfere with tumor growth by inhibiting angiogenesis
as well as tumor cell proliferation. Sunitinib appears to offer greater potency against advanced RCC, perhaps because it inhibits more receptors than sorafenib.
(CCI-779) is an inhibitor of mTOR kinase (mammalian target of rapamycin
) that was shown to prolong overall survival vs. interferon-α in patients with previously untreated metastatic renal cell carcinoma with three or more poor prognostic features. It was approved in May 2007 by the US FDA, and approved in EU in Nov 2007.
2007: Sunitinib
; The first Phase III study comparing an RTKI with cytokine therapy was published in the New England Journal of Medicine
. This study showed that Sunitinib
offered superior efficacy compared with interferon-α. Progression-free survival (primary endpoint) was more than doubled. The benefit for sunitinib was significant across all major patient subgroups, including those with a poor prognosis at baseline. 28% of sunitinib patients had significant tumor shrinkage compared with only 5% of patients who received interferon-α. Although overall survival data are not yet mature, there is a clear trend toward improved survival with sunitinib. Patients receiving sunitinib also reported a significantly better quality of life than those treated with IFNa.
June 2008: Good results were reported for Thalomid and Revlimid in trials for the treatment of renal cell carcinoma.
March 2009 : Everolimus
(Afinitor) (an oral once-daily inhibitor of mTOR) was approved by the US FDA for first treatment for patients with advanced kidney cancer after failure of either sunitinib or sorafenib.
2009: Carfilzomib
, a novel proteasome inhibitor, shows efficacy and is well tolerated in relapsed RCC.
In 2010 a Phase III trial of Axitinib
for previously treated metastatic renal cell carcinoma (mRCC) showed significantly extended progression-free survival when compared to sorafenib
.
, have shown promising results in phase 2 trials for treatment of renal cell carcinoma. However, issues of tumor immunosuppression
and lack of identified tumor-associated antigens must be addressed before vaccine therapy can be applied successfully in advanced renal cell cancer.
stage of renal cell carcinoma occurs when the disease invades and spreads to other organs. It is most likely to spread to neighboring lymph nodes, the lungs, the liver, the bones, or the brain.
Metastatic renal cell carcinoma presents a special challenge to oncologists, as about 70% of patients develop metastases during the course of their disease, and 5 year survival for patients with metastatic renal cell carcinoma is between 5 and 15%, although it is much improved if metastatectomy and nephrectomy
to remove all visible disease is performed. Even if metastases are not removed, cytoreductive nephrectomy is sometimes used in the treatment of metastatic renal cell carcinoma, and at least one study has supported the use of this operation in "some cases", citing improved response rates to interleukin-2 immunotherapy
and modestly prolonged survival.
Radiotherapy and chemotherapy
have less of a role in the treatment of renal cell carcinoma than in other malignancies; but they are still sometimes used in treatment of the metastatic disease. Radiotherapy is used in in cases of bone metastases, to reduce pain and lower the risk of pathologic fracture
, in patients with brain metastases, and to palliate symptoms of metastatic disease to the liver, adrenals, or lungs.
Interleukin-2 has been the standard of care since the 1990s in metastatic renal cell carcinoma, as, although response rates are low [7-16%], about half of patients that respond have long term disease-free survival, and some of these patients may be completely cured. However,the side effects of interleukin-2 are severe, including decreased neutrophil function, increased risk of disseminated infection, including central venous catheter
infections, septicaemia, bacterial endocarditis, and capillary leak syndrome, which can result in myocardial infarction
, renal failure
, angina
, hypotension
, reduced organ perfusion, altered mental status, pulmonary failure requiring intubation
, cardiac arrhythmias, edema
, and gastrointestinal bleeding.
The use of proleukin can also result in lethargy and somnolence; if interleukin-2 therapy is not discontinued lethargy may progress to coma. Interleukin-2 can also worsen preexisting autoimmune diseases. Neurological side effects can also occur, and include ataxia
, cortical blindness, hallucinations, psychosis
, speech problems, and coma. Other side effects include abdominal pain
, rigors, fever
, malaise
, asthenia, acidosis
, tachycardia
, vasodilatation, diarrhea
, vomiting
, mouth sores, loss of appetite, dermatitis
, dyspnea
, thrombocytopenia
, and anaemia. Therefore, patients must be in good health with normal cardiovascular, hepatic, pulmonary,and neurological function to be treated with interleukin-2.
Recently, targeted therapies such as torisel, nexavar, sutent, votrient, and bevacizumab
, have been developed, and all are now approved for the treatment of metastatic renal cell carcinoma. The three to five years up to 2009 saw dramatic improvements in treatment for those with metastatic renal cell carcinoma. However, despite these improvements in therapy, overall survival remains poor.
Currently, tumor vaccines and chemotherapeutic, biologic, and immunologic agents are being researched in the treatment of metastatic renal cell carcinoma, and some appear promising. It is not known whether or not detecting metastases earlier improves survival or response to treatment.
There is currently no established adjuvant therapy for renal cell carcinoma, although there have been a number of clinical trials exploring the effectiveness of various potential treatments.
The use of non-specific cytokines has so far been shown to be ineffective. Unlike most other cancers, renal cell carcinoma is resistant to most cytotoxic and cytostatic agents,which severely limits possible effective adjuvant therapy. Trials of "cancer vaccines", radiotherapy, chemotherapy, immunotherapy, or biologic therapies (i.e. nexavar, sutent) have been met with little success,and currently the standard of care for completely resected high-risk renal cell carcinoma is close observation with no other therapy. There does appear to be some evidence that if there cancer is incompletely resected (positive surgical margins,adrenal involvement,vena caval involvement) radiotherapy reduces the risk of invasive local disease,but data is lacking on that as well.
There have also been a number of trials of Autolymphocyte therapy (ALT) which have shown varying degrees of efficacy.
ALT is a form of outpatient adoptive immunotherapy utilizing autologous ex vivo activated T-cells accompanied by high dose cimetidine.
Paul Grawitz
first described renal cell carcinoma in 1883.
Kidney cancer
Kidney cancer is a type of cancer that starts in the cells in the kidney.The two most common types of kidney cancer are renal cell carcinoma and urothelial cell carcinoma of the renal pelvis...
that originates in the lining of the proximal convoluted tubule
Proximal tubule
The proximal tubule is the portion of the duct system of the nephron of the kidney which leads from Bowman's capsule to the loop of Henle.-Structure and appearance:...
, the very small tubes in the kidney that filter the blood and remove waste products. RCC is the most common type of kidney cancer in adults, responsible for approximately 80% of cases. It is also known to be the most lethal of all the genitourinary tumors. Initial treatment is most commonly a radical or partial nephrectomy
Nephrectomy
Nephrectomy is the surgical removal of a kidney.-History:The first successful nephrectomy was performed by the German surgeon Gustav Simon on August 2, 1869 in Heidelberg. Simon practiced the operation beforehand in animal experiments...
and remains the mainstay of curative treatment. Where the tumor is confined to the renal parenchyma, the 5-year survival rate is 60-70%, but this is lowered considerably where metastases have spread. It is resistant to radiation therapy
Radiation therapy
Radiation therapy , radiation oncology, or radiotherapy , sometimes abbreviated to XRT or DXT, is the medical use of ionizing radiation, generally as part of cancer treatment to control malignant cells.Radiation therapy is commonly applied to the cancerous tumor because of its ability to control...
and chemotherapy
Chemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
, although some cases respond to immunotherapy
Immunotherapy
Immunotherapy is a medical term defined as the "treatment of disease by inducing, enhancing, or suppressing an immune response". Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies. While immunotherapies that reduce or suppress are...
. Targeted cancer therapies such as sunitinib
Sunitinib
Sunitinib is an oral, small-molecule, multi-targeted receptor tyrosine kinase inhibitor that was approved by the FDA for the treatment of renal cell carcinoma and imatinib-resistant gastrointestinal stromal tumor on January 26, 2006...
, temsirolimus
Temsirolimus
Temsirolimus is an intravenous drug for the treatment of renal cell carcinoma , developed by Wyeth Pharmaceuticals and approved by the U.S. Food and Drug Administration in late May 2007, and was also approved by the European Medicines Agency on November 2007...
, bevacizumab
Bevacizumab
Bevacizumab is a drug that blocks angiogenesis, the growth of new blood vessels. It is commonly used to treat various cancers, including colorectal, lung, breast, kidney, and glioblastomas....
, interferon-alpha, and possibly sorafenib
Sorafenib
Sorafenib , is a drug approved for the treatment of primary kidney cancer and advanced primary liver cancer ....
have improved the outlook for RCC (progression-free survival), although they have not yet demonstrated improved survival.
Signs and symptoms
A wide range of symptoms can be present with renal carcinoma depending on which areas of the body have been affected. The classic triad is hematuriaHematuria
In medicine, hematuria, or haematuria, is the presence of red blood cells in the urine. It may be idiopathic and/or benign, or it can be a sign that there is a kidney stone or a tumor in the urinary tract , ranging from trivial to lethal...
(blood in the urine), flank pain and an abdominal mass. This triad only occurs in 10-15% of cases, and is generally indicative of more advanced disease. Today, the majority of renal tumors are asymptomatic and are detected incidentally on imaging, usually for an unrelated cause.
Signs may include:
- abnormal urine color (dark, rusty, or brown) due to blood in the urine (found in 60% of cases)
- loin pain (found in 40% of cases)
- abdominal mass (25% of cases)
- malaise, weight loss or anorexia (30% of cases)
- polycythemiaPolycythemiaPolycythemia is a disease state in which the proportion of blood volume that is occupied by red blood cells increases...
(5% of cases) - anemiaAnemiaAnemia is a decrease in number of red blood cells or less than the normal quantity of hemoglobin in the blood. However, it can include decreased oxygen-binding ability of each hemoglobin molecule due to deformity or lack in numerical development as in some other types of hemoglobin...
resulting from depression of erythropoietinErythropoietinErythropoietin, or its alternatives erythropoetin or erthropoyetin or EPO, is a glycoprotein hormone that controls erythropoiesis, or red blood cell production...
(30% of cases) Also, there may be erythrocytosis (increased production of red blood cellRed blood cellRed blood cells are the most common type of blood cell and the vertebrate organism's principal means of delivering oxygen to the body tissues via the blood flow through the circulatory system...
s) due to increased erythropoietin secretion. - the presenting symptom may be due to metastatic disease, such as a pathologic fracture of the hip due to a metastasis to the bone
- varicoceleVaricoceleVaricocele , also known as varicoscele or varicose seal, is an abnormal enlargement of the vein that is in the scrotum draining the testicles. The testicular blood vessels originate in the abdomen and course down through the inguinal canal as part of the spermatic cord on their way to the testis...
, the enlargement of one testicle, usually on the left (2% of cases). This is due to blockage of the left testicular veinTesticular veinThe testicular vein , the male gonadal vein, carries deoxygenated blood from its corresponding testis to the inferior vena cava or one of its tributaries...
by tumor invasion of the left renal veinRenal veinThe renal veins are veins that drain the kidney. They connect the kidney to the inferior vena cava.It is usually singular to each kidney, except in the condition "multiple renal veins".It also divides into 2 divisions upon entering the kidney:...
; this typically does not occur on the right as the right gonadal vein drains directly into the inferior vena cavaInferior vena cavaThe inferior vena cava , also known as the posterior vena cava, is the large vein that carries de-oxygenated blood from the lower half of the body into the right atrium of the heart....
. - vision abnormalities
- pallor or plethora
- hirsutismHirsutismHirsutism or frazonism is the excessive hairiness on women in those parts of the body where terminal hair does not normally occur or is minimal - for example, a beard or chest hair. It refers to a male pattern of body hair and it is therefore primarily of cosmetic and psychological concern...
- excessive hair growth (females) - constipation
- hypertensionHypertensionHypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
(high blood pressure) resulting from secretion of reninReninRenin , also known as an angiotensinogenase, is an enzyme that participates in the body's renin-angiotensin system -- also known as the Renin-Angiotensin-Aldosterone Axis -- that mediates extracellular volume , and arterial vasoconstriction...
by the tumour (30% of cases) - elevated calcium levels (hypercalcemia)
- Stauffer syndromeStauffer syndromeStauffer syndrome was described initially by Maurice H. Stauffer, M.D., a gastroenterologist at the Mayo Clinic in Rochester, MN. This condition is a constellation of signs and symptoms of liver dysfunction that arise due to presence of renal cell carcinoma, and, more rarely, in connection with...
- paraneoplastic, non-metastatic liverLiverThe liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion...
disease - night sweats
- severe weight loss
Patients may also experience the following symptoms:
- recurrent feverFeverFever is a common medical sign characterized by an elevation of temperature above the normal range of due to an increase in the body temperature regulatory set-point. This increase in set-point triggers increased muscle tone and shivering.As a person's temperature increases, there is, in...
s which occur in 9% of the patients - cold intolerance
- back pain
- chronic fatigue
- leg and ankle swelling
- loss of appetite
Classification
- clear cell renal cell carcinoma (VHLVon Hippel-Lindau tumor suppressorThe Von Hippel–Lindau tumor suppressor also known as pVHL is a protein that in humans is encoded by the VHL gene. Mutations of the VHL gene are associated with Von Hippel–Lindau disease....
, PBRM1PBRM1Protein polybromo-1 also known as BRG1-associated factor 180 is a protein that in humans is encoded by the PBRM1 gene.- Structure and function :...
and others on chromosome 3) - Papillary Renal Cell Carcinoma (METC-METc-Met is a proto-oncogene that encodes a protein known as hepatocyte growth factor receptor . The hepatocyte growth factor receptor protein possesses tyrosine-kinase activity...
, PRCCPRCC (gene)Proline-rich protein PRCC is a protein that in humans is encoded by the PRCC gene.-Further reading:...
) - chromophobeChromophobeThe term chromophobe refers to histological structures which do not stain readily, and thus appear more relatively pale under the microscope—hence their "fear" of "color" .-Cancer:...
renal cell carcinoma - collecting duct carcinoma
- clear cell papillary renal cell carcinomaClear cell papillary renal cell carcinomaClear cell papillary renal cell carcinoma, abbreviated CCPRCC and also known as clear cell tubulopapillary renal cell carcinoma, is a newly described type of kidney cancer that has microscopic morphologic features of papillary renal cell carcinoma and clear cell renal cell carcinoma, yet is...
Renal epithelial neoplasms have characteristic cytogenetic aberrations that can aid in classification. See also Atlas of Genetics and Cytogenetics in Oncology and Haematology.
- clear cell carcinoma: loss of 3p
- papillary carcinoma: trisomy 7, 16, 17
- chromophobe carcinoma: hypodiploid with loss of chromosomes 1, 2, 6, 10, 13, 17, 21
Array-based karyotyping can be used to identify characteristic chromosomal aberrations in renal tumors with challenging morphology. Array-based karyotyping performs well on paraffin embedded tumors and is amenable to routine clinical use. See also Virtual Karyotype
Virtual Karyotype
Virtual karyotype detects genomic copy number variations at a higher resolution level than conventional karyotyping or chromosome-based comparative genomic hybridization .-Background:...
for CLIA certified laboratories offering array-based karyotyping of solid tumors.
Other associated genes include TRC8, OGG1, HNF1A
HNF1A
HNF1 homeobox A , also known as HNF1A, is a human gene.The protein encoded by this gene is a transcription factor that is highly expressed in the liver and is involved in the regulation of the expression of several liver-specific genes.-Interactions:HNF1A has been shown to interact with PCAF, Src,...
, HNF1B
HNF1B
HNF1 homeobox B , also known as HNF1B or transcription factor 2 , is a human gene.-Further reading:...
, TFE3
TFE3
Transcription factor E3 is a protein that in humans is encoded by the TFE3 gene.-Interactions:TFE3 has been shown to interact with E2F3, Mothers against decapentaplegic homolog 3 and Microphthalmia-associated transcription factor.-Further reading:...
, RCCP3, and RCC17.
Epidemiology
The incidence of renal cell cancer has been rising steadily. Nearly 51190 new diagnoses and 12890 deaths reported in the United States in 2007. It is more common in men than women: the male-to-female ratio is 1.6:1 and has been decreasing over the last decade. Blacks have a slightly higher rate of renal cell cancer than whites. The reasons for this are not clear. Note: in epidemiology, RCC is registered together with renal pelvis carcinoma, which is predominantly transitional cell type.In Europe the incidence of RCC has doubled in the period from 1975 to 2005. RCC accounted for 3777 deaths in the UK in 2006; male 2372, female 1820.
Risk factors
Cigarette smoking and obesity are the strongest known risk factorsRisk factors
A risk factor is a concept in finance theory such as the CAPM, APT and other theories that use pricing kernels. In these models, the rate of return of an asset is a random variable whose realization in any time period is a linear combination of other random variables plus a disturbance term or...
. Hypertension
Hypertension
Hypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
and a family history of the disease are also risk factors. Occupational exposure to cadmium is a risk factor.
Dialysis
Dialysis
In medicine, dialysis is a process for removing waste and excess water from the blood, and is primarily used to provide an artificial replacement for lost kidney function in people with renal failure...
patients with acquired cystic disease of the kidney showed a 30 times greater risk than in the general population for developing RCC.
Exposure to asbestos, polycyclic aromatic hydrocarbons, gasoline has not been shown to be consistently associated with RCC risk.
Patients with certain inherited disorders such as von Hippel-Lindau disease
Von Hippel-Lindau disease
Von Hippel–Lindau is a rare, autosomal dominant genetic condition in which hemangioblastomas are found in the cerebellum, spinal cord, kidney and retina. These are associated with several pathologies including renal angioma, renal cell carcinoma and pheochromocytoma...
, hereditary papillary renal cancer, a hereditary leiomyoma RCC syndrome and Birt-Hogg-Dubé syndrome, show an enhanced risk of RCC. Also, patients with sickle cell trait
Sickle cell trait
Sickle cell trait describes a condition in which a person has one abnormal allele of the hemoglobin beta gene , but does not display the severe symptoms of sickle cell disease that occur in a person who has two copies of that allele...
are predisposed to developing Renal medullary carcinoma
Renal medullary carcinoma
Renal medullary carcinoma is a rare type of cancer that affects the kidney. It tends to be aggressive, difficult to treat, and is often metastatic at the time of diagnosis...
.
Hysterectomy
Hysterectomy
A hysterectomy is the surgical removal of the uterus, usually performed by a gynecologist. Hysterectomy may be total or partial...
is associated with an approximately doubled risk. Hormonal factors or injury of the ureter during surgery were considered as possible causes.
Diagnosis
An accurate diagnosis may be difficult to establish given that the early stages of renal cancer are asymptomatic.The first steps taken in order to diagnose this condition are observing any of the signs and symptoms, and an anamnesis
Medical history
The medical history or anamnesis of a patient is information gained by a physician by asking specific questions, either of the patient or of other people who know the person and can give suitable information , with the aim of obtaining information useful in formulating a diagnosis and providing...
(the detailed medical review of past health state) to evaluate any risk factors. Upon physical examination
Physical examination
Physical examination or clinical examination is the process by which a doctor investigates the body of a patient for signs of disease. It generally follows the taking of the medical history — an account of the symptoms as experienced by the patient...
, palpation of the abdomen may reveal the presence of a mass or an organ enlargement.
However, the main diagnostic tool for detecting renal cell carcinoma is ultrasound
Medical ultrasonography
Diagnostic sonography is an ultrasound-based diagnostic imaging technique used for visualizing subcutaneous body structures including tendons, muscles, joints, vessels and internal organs for possible pathology or lesions...
of the kidneys. If the ultrasound shows a mass or cyst, a subsequent abdominal CT is the optimal test for diagnosis and staging
Cancer staging
The stage of a cancer is a description of the extent the cancer has spread. The stage often takes into account the size of a tumor, how deeply it has penetrated, whether it has invaded adjacent organs, how many lymph nodes it has metastasized to , and whether it has spread to distant organs...
.
Radiology
The characteristic appearance of renal cell carcinoma (RCC) is a solid renal lesion which disturbs the renal contour. It will frequently have an irregular or lobulated margin. Traditionally 85 to 90% of solid renal masses will turn out to be RCC but this number may be decreasing as renal masses are being found at smaller and smaller sizes with larger numbers of benign lesions. Ten percent of RCC will contain calcifications, and some contain macroscopic fat (likely due to invasion and encasement of the perirenal fat).Renal cell carcinoma may also be cystic. As there are several benign cystic renal lesions (simple renal cyst, hemorrhagic renal cyst, multilocular cystic nephroma, polycystic kidney disease), it may occasionally be difficult for the radiologist to differentiate a benign cystic lesion from a malignant one. A classification system for cystic renal lesions that classifies them based specific imaging features into groups that are benign and those that need surgical resection is available.
Percutaneous biopsy can be performed by a radiologist using ultrasound
Medical ultrasonography
Diagnostic sonography is an ultrasound-based diagnostic imaging technique used for visualizing subcutaneous body structures including tendons, muscles, joints, vessels and internal organs for possible pathology or lesions...
or computed tomography
Computed tomography
X-ray computed tomography or Computer tomography , is a medical imaging method employing tomography created by computer processing...
to guide sampling of the tumor for the purpose of diagnosis by pathology. However this is not routinely performed because when the typical imaging features of renal cell carcinoma are present, the possibility of an incorrectly negative result together with the risk of a medical complication to the patient make it unfavorable from a risk-benefit perspective. This is not completely accurate, there are new experimental treatments.
Staging
The stagingCancer staging
The stage of a cancer is a description of the extent the cancer has spread. The stage often takes into account the size of a tumor, how deeply it has penetrated, whether it has invaded adjacent organs, how many lymph nodes it has metastasized to , and whether it has spread to distant organs...
of renal cell carcinoma is the most important factor in predicting its prognosis. Staging can follow the TNM staging system, where the size and extent of the tumour (T), involvement of lymph nodes (N) and metastases (M) are classified separately. Also, it can use overall stage grouping into stage I-IV, with the 1997 revision of AJCC described below:
| Stage I | Tumor of a diameter of 7 cm (approx. 2 inches) or smaller, and limited to the kidney. No lymph node involvement or metastases to distant organs. |
| Stage II | Tumor larger than 7.0 cm but still limited to the kidney. No lymph node involvement or metastases to distant organs. |
| Stage III any of the following |
Tumor of any size with involvement of a nearby lymph node but no metastases to distant organs. Tumor of this stage may be with or without spread to fatty tissue around the kidney, with or without spread into the large veins leading from the kidney to the heart. |
| Tumor with spread to fatty tissue around the kidney and/or spread into the large veins leading from the kidney to the heart, but without spread to any lymph nodes or other organs. | |
| Stage IV any of the following |
Tumor that has spread directly through the fatty tissue and the fascia ligament-like tissue that surrounds the kidney. |
| Involvement of more than one lymph node near the kidney | |
| Involvement of any lymph node not near the kidney | |
| Distant metastases, such as in the lungs, bone, or brain. |
At diagnosis, 30% of renal cell carcinomas have spread to the ipsilateral renal vein, and 5-10% have continued into the inferior vena cava.
Histopathology
The renal cell carcinoma may present reddened areas where blood vessels have bled, and cysts containing watery fluids. The body of the tumor shows large blood vessels that have walls composed of cancerous cells.
Gross examination
Gross examination
Gross examination or "grossing" is the process by which pathology specimens are inspected with the bare eye to obtain diagnostic information, while being processed for further microscopic examination....
often shows a yellowish, multilobulated tumor in the renal cortex, which frequently contains zones of necrosis, hemorrhage and scarring.
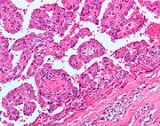
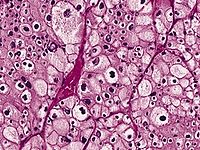
Light microscopy shows tumor cells forming cords, papillae, tubules or nests, and are atypical, polygonal and large. Also, the cells that make up a renal carcinoma may be clear, granular, mixed clear and granular or sarcomatoid or spindle type. Recent studies have brought to attention that the type of cancerous cells and the aggressiveness of the condition are closely related.Because these cells accumulate glycogen
Glycogen
Glycogen is a molecule that serves as the secondary long-term energy storage in animal and fungal cells, with the primary energy stores being held in adipose tissue...
and lipid
Lipid
Lipids constitute a broad group of naturally occurring molecules that include fats, waxes, sterols, fat-soluble vitamins , monoglycerides, diglycerides, triglycerides, phospholipids, and others...
s, their cytoplasm appear "clear", the nuclei remain in the middle of the cells, and the cellular membrane is evident. Some cells may be smaller, with eosinophilic cytoplasm, resembling normal tubular cells. The stroma is reduced, but well vascularized. The tumor compresses the surrounding parenchyma, producing a pseudocapsule.
The clear cells are thought to be the least likely to spread and usually respond more favorably to treatment. However, most of the tumors contain a mixture of cells. The most aggressive stage of renal cancer is believed to be the one in which the tumor is mixed, containing both clear and granular cells.
Prognosis
A study in TurkeyTurkey
Turkey , known officially as the Republic of Turkey , is a Eurasian country located in Western Asia and in East Thrace in Southeastern Europe...
that used the 1997 AJCC staging system estimated the five year survival rate to be 90% for stage I, 51% for stage II, 22% for stage III and 4.6% for stage IV. The same study estimated the median survival time to be 7.7 years for stage I, 5.0 years for stage II, 3.1 years for stage III and 1.1 years for stage IV.
For those that have tumor recurrence after surgery, the prognosis is generally poor. Renal cell carcinoma does not generally respond to chemotherapy or radiation. Immunotherapy, which attempts to induce the body to attack the remaining cancer cells, has shown promise. Recent trials are testing newer agents, though the current complete remission rate with these approaches are still low, around 12-20% in most series. Most recently, treatment with tyrosine kinase inhibitors including nexavar, pazopanib
Pazopanib
Pazopanib is a potent and selective multi-targeted receptor tyrosine kinase inhibitor of VEGFR-1, VEGFR-2, VEGFR-3, PDGFR-a/β, and c-kit that blocks tumor growth and inhibits angiogenesis. It has been approved for renal cell carcinoma by the U.S. Food and Drug Administration. Pazopanib may also be...
, and rapamycin have shown promise in improving the prognosis for advanced RCC since 2004.
Treatment
If it is only in the kidneys, which is about 40% of cases, it can be cured roughly 90% of the time with surgerySurgery
Surgery is an ancient medical specialty that uses operative manual and instrumental techniques on a patient to investigate and/or treat a pathological condition such as disease or injury, or to help improve bodily function or appearance.An act of performing surgery may be called a surgical...
. If it has spread outside of the kidneys, often into the lymph nodes or the main vein of the kidney, then it must be treated with adjunctive therapy, including cytoreductive surgery. RCC is resistant to chemotherapy and radiotherapy in most cases, but does respond well to immunotherapy with interleukin-2 or interferon-alpha, biologic, or targeted therapy. In early stage cases, cryotherapy and surgery are the preferred options.
Watchful waiting
Small renal tumors (< 4 cm) are treated increasingly by way of partial nephrectomyNephrectomy
Nephrectomy is the surgical removal of a kidney.-History:The first successful nephrectomy was performed by the German surgeon Gustav Simon on August 2, 1869 in Heidelberg. Simon practiced the operation beforehand in animal experiments...
when possible. Most of these small renal masses manifest indolent biological behavior with excellent prognosis. More centers of excellence are incorporating needle biopsy to confirm the presence of malignant histology prior to recommending definitive surgical extirpation. In the elderly, patients with co-morbidities and in poor surgical candidates, small renal tumors may be monitored carefully with serial imaging. Most clinicians conservatively follow tumors up to a size threshold between 3 and 5 cm, beyond which the risk of distant spread (metastases) is about 5%.
Cryoablation
Cryoablation is used in a variety of clinical applications using hollow needles (cryoprobes) through which cooled, thermally conductive, fluids are circulated. Cryoprobes are inserted into or placed adjacent to tissue which is determined to be diseased in such a way that ablation will provide correction yielding benefit to the patient. When the probes are in place, the cryogenic freezing unit removes heat ("cools") from the tip of the probe and by extension from the surrounding tissues.The most common application of cryoablation is to ablate solid tumors found in the lung, liver, breast, kidney and prostate. The use in prostate and renal cryoablation are the most common. Although sometimes applied through laparoscopic or open surgical approaches, most often cryoablation is performed percutaneously (through the skin and into the target tissue containing the tumor).
Surgery
Nephrectomy
Nephrectomy is the surgical removal of a kidney.-History:The first successful nephrectomy was performed by the German surgeon Gustav Simon on August 2, 1869 in Heidelberg. Simon practiced the operation beforehand in animal experiments...
) is recommended. This may include removal of the adrenal gland, retroperitoneal lymph nodes, and possibly tissues involved by direct extension (invasion) of the tumor into the surrounding tissues. In cases where the tumor has spread into the renal vein, inferior vena cava, and possibly the right atrium, this portion of the tumor can be surgically removed, as well. In cases of known metastases, surgical resection of the kidney ("cytoreductive nephrectomy") may improve survival, as well as resection of a solitary metastatic lesion. Kidneys are sometimes embolized
Embolization
Embolization is a non-surgical, minimally-invasive procedure performed by an interventional radiologist and interventional neuroradiologists. It involves the selective occlusion of blood vessels by purposely introducing emboli.-Therapeutic applications:...
prior to surgery to minimize blood loss (see image).
Surgery is increasingly performed via laparoscopic
Laparoscopy
Laparoscopy is an operation performed in the abdomen or pelvis through small incisions with the aid of a camera...
techniques. These have the advantage of being less of a burden for the patient and the disease-free survival is comparable to that of open surgery. For small exophytic lesions that do not extensively involve the major vessels or urinary collecting system, a partial nephrectomy (also referred to as "nephron sparing surgery") can be performed. This may involve temporarily stopping blood flow to the kidney while the mass is removed as well as renal cooling with an ice slush. Mannitol
Mannitol
Mannitol is a white, crystalline organic compound with the formula . This polyol is used as an osmotic diuretic agent and a weak renal vasodilator...
can also be administered to help limit damage to the kidney. This is usually done through an open incision although smaller lesions can be done laparoscopically with or without robotic assistance.
Laparoscopic cryotherapy
Cryotherapy
Cryotherapy is the local or general use of low temperatures in medical therapy or the removal of heat from a body part. The term "cryotherapy" comes from the Greek cryo meaning cold and the word therapy meaning cure...
can also be done on smaller lesions. Typically a biopsy is taken at the time of treatment. Intraoperative ultrasound may be used to help guide placement of the freezing probes. Two freeze/thaw cycles are then performed to kill the tumor cells. As the tumor is not removed followup is more complicated (see below) and overall disease free rates are not as good as those obtained with surgical removal.
Percutaneous therapies
PercutaneousPercutaneous
In surgery, percutaneous pertains to any medical procedure where access to inner organs or other tissue is done via needle-puncture of the skin, rather than by using an "open" approach where inner organs or tissue are exposed .The percutaneous approach is commonly used in vascular procedures...
, image-guided therapies, usually managed by radiologists, are being offered to patients with localized tumor, but who are not good candidates for a surgical procedure. This sort of procedure involves placing a probe through the skin and into the tumor using real-time imaging of both the probe tip and the tumor by computed tomography
Computed tomography
X-ray computed tomography or Computer tomography , is a medical imaging method employing tomography created by computer processing...
, ultrasound
Ultrasound
Ultrasound is cyclic sound pressure with a frequency greater than the upper limit of human hearing. Ultrasound is thus not separated from "normal" sound based on differences in physical properties, only the fact that humans cannot hear it. Although this limit varies from person to person, it is...
, or even magnetic resonance imaging
Magnetic resonance imaging
Magnetic resonance imaging , nuclear magnetic resonance imaging , or magnetic resonance tomography is a medical imaging technique used in radiology to visualize detailed internal structures...
guidance, and then destroying the tumor with heat (radiofrequency ablation
Radiofrequency ablation
Radio frequency ablation is a medical procedure where part of the electrical conduction system of the heart, tumor or other dysfunctional tissue is ablated using the heat generated from the high frequency alternating current to treat a medical disorder...
) or cold (cryotherapy
Cryotherapy
Cryotherapy is the local or general use of low temperatures in medical therapy or the removal of heat from a body part. The term "cryotherapy" comes from the Greek cryo meaning cold and the word therapy meaning cure...
). These modalities are at a disadvantage compared to traditional surgery in that pathologic confirmation of complete tumor destruction is not possible. Therefore, long-term follow-up is crucial to assess completeness of tumour ablation.
Medications for advanced or metastatic cases
RCC "elicits an immune response, which occasionally results in dramatic spontaneous remissions." This has encouraged a strategy of using immunomodulating therapies, such as cancer vaccines and interleukin-2 (IL-2), to reproduce this response. IL-2 has produced "durable remissions" in a small number of patients, but with substantial toxicity. Another strategy is to restore the function of the VHL gene, which is to destroy proteins that promote inappropriate vascularization. BevacizumabBevacizumab
Bevacizumab is a drug that blocks angiogenesis, the growth of new blood vessels. It is commonly used to treat various cancers, including colorectal, lung, breast, kidney, and glioblastomas....
, an antibody to VEGF
Vascular endothelial growth factor
Vascular endothelial growth factor is a signal protein produced by cells that stimulates vasculogenesis and angiogenesis. It is part of the system that restores the oxygen supply to tissues when blood circulation is inadequate....
, has significantly prolonged time to progression, but phase 3 trials have not been published. Sunitinib (Sutent), sorafenib (Nexavar), and temsirolimus, which are small-molecule inhibitors of proteins, have been approved by the U.S. F.D.A.
Treatment with tyrosine kinase inhibitors including Nexavar, pazopanib
Pazopanib
Pazopanib is a potent and selective multi-targeted receptor tyrosine kinase inhibitor of VEGFR-1, VEGFR-2, VEGFR-3, PDGFR-a/β, and c-kit that blocks tumor growth and inhibits angiogenesis. It has been approved for renal cell carcinoma by the U.S. Food and Drug Administration. Pazopanib may also be...
, and rapamycin have shown promise in improving the prognosis for advanced RCC since 2004.
Sorafenib
Sorafenib
Sorafenib , is a drug approved for the treatment of primary kidney cancer and advanced primary liver cancer ....
(Nexavar), a protein kinase inhibitor, was FDA approved in December 2005 for treatment of advanced renal cell cancer.
A month later, Sunitinib
Sunitinib
Sunitinib is an oral, small-molecule, multi-targeted receptor tyrosine kinase inhibitor that was approved by the FDA for the treatment of renal cell carcinoma and imatinib-resistant gastrointestinal stromal tumor on January 26, 2006...
(Sutent) was approved as well. Sunitinib (an oral, small-molecule, multi-targeted (RTK) inhibitor) and sorafenib both interfere with tumor growth by inhibiting angiogenesis
Angiogenesis
Angiogenesis is the physiological process involving the growth of new blood vessels from pre-existing vessels. Though there has been some debate over terminology, vasculogenesis is the term used for spontaneous blood-vessel formation, and intussusception is the term for the formation of new blood...
as well as tumor cell proliferation. Sunitinib appears to offer greater potency against advanced RCC, perhaps because it inhibits more receptors than sorafenib.
2007 on
TemsirolimusTemsirolimus
Temsirolimus is an intravenous drug for the treatment of renal cell carcinoma , developed by Wyeth Pharmaceuticals and approved by the U.S. Food and Drug Administration in late May 2007, and was also approved by the European Medicines Agency on November 2007...
(CCI-779) is an inhibitor of mTOR kinase (mammalian target of rapamycin
Mammalian target of rapamycin
The mammalian target of rapamycin also known as mechanistic target of rapamycin or FK506 binding protein 12-rapamycin associated protein 1 is a protein which in humans is encoded by the FRAP1 gene...
) that was shown to prolong overall survival vs. interferon-α in patients with previously untreated metastatic renal cell carcinoma with three or more poor prognostic features. It was approved in May 2007 by the US FDA, and approved in EU in Nov 2007.
2007: Sunitinib
Sunitinib
Sunitinib is an oral, small-molecule, multi-targeted receptor tyrosine kinase inhibitor that was approved by the FDA for the treatment of renal cell carcinoma and imatinib-resistant gastrointestinal stromal tumor on January 26, 2006...
; The first Phase III study comparing an RTKI with cytokine therapy was published in the New England Journal of Medicine
New England Journal of Medicine
The New England Journal of Medicine is an English-language peer-reviewed medical journal published by the Massachusetts Medical Society. It describes itself as the oldest continuously published medical journal in the world.-History:...
. This study showed that Sunitinib
Sunitinib
Sunitinib is an oral, small-molecule, multi-targeted receptor tyrosine kinase inhibitor that was approved by the FDA for the treatment of renal cell carcinoma and imatinib-resistant gastrointestinal stromal tumor on January 26, 2006...
offered superior efficacy compared with interferon-α. Progression-free survival (primary endpoint) was more than doubled. The benefit for sunitinib was significant across all major patient subgroups, including those with a poor prognosis at baseline. 28% of sunitinib patients had significant tumor shrinkage compared with only 5% of patients who received interferon-α. Although overall survival data are not yet mature, there is a clear trend toward improved survival with sunitinib. Patients receiving sunitinib also reported a significantly better quality of life than those treated with IFNa.
June 2008: Good results were reported for Thalomid and Revlimid in trials for the treatment of renal cell carcinoma.
March 2009 : Everolimus
Everolimus
Everolimus is the 40-O- derivative of sirolimus and works similarly to sirolimus as an mTOR inhibitor....
(Afinitor) (an oral once-daily inhibitor of mTOR) was approved by the US FDA for first treatment for patients with advanced kidney cancer after failure of either sunitinib or sorafenib.
2009: Carfilzomib
Carfilzomib
Carfilzomib is a tetrapeptide epoxyketone and a selective proteasome inhibitor. It is an analog of epoxomicin.-Discovery and Early Development:...
, a novel proteasome inhibitor, shows efficacy and is well tolerated in relapsed RCC.
In 2010 a Phase III trial of Axitinib
Axitinib
Axitinib is a small molecule tyrosine kinase inhibitor under development by Pfizer. It inhibits multiple targets, including VEGFR-1, VEGFR-2, VEGFR-3, platelet derived growth factor receptor , and cKIT...
for previously treated metastatic renal cell carcinoma (mRCC) showed significantly extended progression-free survival when compared to sorafenib
Sorafenib
Sorafenib , is a drug approved for the treatment of primary kidney cancer and advanced primary liver cancer ....
.
Chemotherapy
Most of the currently available cytostatics are ineffective for the treatment of RCC. Their use can not be recommended for the treatment of patients with metastasized RCC,as response rates are very low,often just 5-15%,and most responses are short lived. The use of Tyrosine Kinase (TK) inhibitors, such as Sunitinib and Sorafenib, and Temsirolimus are described in a different sectionVaccine
Cancer vaccines, such as TroVaxTroVax
TroVax is a cancer vaccine being developed by Oxford BioMedica. No cancer vaccines have been proven to cure cancer or extend life yet, but TroVax is recruiting patients for 3 human trials.TroVax uses a tumor-associated antigen, 5T4, with a pox virus vector...
, have shown promising results in phase 2 trials for treatment of renal cell carcinoma. However, issues of tumor immunosuppression
Immunosuppression
Immunosuppression involves an act that reduces the activation or efficacy of the immune system. Some portions of the immune system itself have immuno-suppressive effects on other parts of the immune system, and immunosuppression may occur as an adverse reaction to treatment of other...
and lack of identified tumor-associated antigens must be addressed before vaccine therapy can be applied successfully in advanced renal cell cancer.
Metastatic renal cell carcinoma
The metastaticMetastasis
Metastasis, or metastatic disease , is the spread of a disease from one organ or part to another non-adjacent organ or part. It was previously thought that only malignant tumor cells and infections have the capacity to metastasize; however, this is being reconsidered due to new research...
stage of renal cell carcinoma occurs when the disease invades and spreads to other organs. It is most likely to spread to neighboring lymph nodes, the lungs, the liver, the bones, or the brain.
Metastatic renal cell carcinoma presents a special challenge to oncologists, as about 70% of patients develop metastases during the course of their disease, and 5 year survival for patients with metastatic renal cell carcinoma is between 5 and 15%, although it is much improved if metastatectomy and nephrectomy
Nephrectomy
Nephrectomy is the surgical removal of a kidney.-History:The first successful nephrectomy was performed by the German surgeon Gustav Simon on August 2, 1869 in Heidelberg. Simon practiced the operation beforehand in animal experiments...
to remove all visible disease is performed. Even if metastases are not removed, cytoreductive nephrectomy is sometimes used in the treatment of metastatic renal cell carcinoma, and at least one study has supported the use of this operation in "some cases", citing improved response rates to interleukin-2 immunotherapy
Immunotherapy
Immunotherapy is a medical term defined as the "treatment of disease by inducing, enhancing, or suppressing an immune response". Immunotherapies designed to elicit or amplify an immune response are classified as activation immunotherapies. While immunotherapies that reduce or suppress are...
and modestly prolonged survival.
Radiotherapy and chemotherapy
Chemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
have less of a role in the treatment of renal cell carcinoma than in other malignancies; but they are still sometimes used in treatment of the metastatic disease. Radiotherapy is used in in cases of bone metastases, to reduce pain and lower the risk of pathologic fracture
Pathologic fracture
A pathologic fracture is a broken bone caused by disease leading to weakness of the bone. This process is most commonly due to osteoporosis, but may also be due to other pathologies such as: cancer, infection, inherited bone disorders,or a bone cyst...
, in patients with brain metastases, and to palliate symptoms of metastatic disease to the liver, adrenals, or lungs.
Interleukin-2 has been the standard of care since the 1990s in metastatic renal cell carcinoma, as, although response rates are low [7-16%], about half of patients that respond have long term disease-free survival, and some of these patients may be completely cured. However,the side effects of interleukin-2 are severe, including decreased neutrophil function, increased risk of disseminated infection, including central venous catheter
Central venous catheter
In medicine, a central venous catheter is a catheter placed into a large vein in the neck , chest or groin...
infections, septicaemia, bacterial endocarditis, and capillary leak syndrome, which can result in myocardial infarction
Myocardial infarction
Myocardial infarction or acute myocardial infarction , commonly known as a heart attack, results from the interruption of blood supply to a part of the heart, causing heart cells to die...
, renal failure
Renal failure
Renal failure or kidney failure describes a medical condition in which the kidneys fail to adequately filter toxins and waste products from the blood...
, angina
Angina
Angina pectoris, commonly known as angina, is chest pain due to ischemia of the heart muscle, generally due to obstruction or spasm of the coronary arteries . Coronary artery disease, the main cause of angina, is due to atherosclerosis of the cardiac arteries...
, hypotension
Hypotension
In physiology and medicine, hypotension is abnormally low blood pressure, especially in the arteries of the systemic circulation. It is best understood as a physiologic state, rather than a disease. It is often associated with shock, though not necessarily indicative of it. Hypotension is the...
, reduced organ perfusion, altered mental status, pulmonary failure requiring intubation
Intubation
Tracheal intubation, usually simply referred to as intubation, is the placement of a flexible plastic or rubber tube into the trachea to maintain an open airway or to serve as a conduit through which to administer certain drugs...
, cardiac arrhythmias, edema
Edema
Edema or oedema ; both words from the Greek , oídēma "swelling"), formerly known as dropsy or hydropsy, is an abnormal accumulation of fluid beneath the skin or in one or more cavities of the body that produces swelling...
, and gastrointestinal bleeding.
The use of proleukin can also result in lethargy and somnolence; if interleukin-2 therapy is not discontinued lethargy may progress to coma. Interleukin-2 can also worsen preexisting autoimmune diseases. Neurological side effects can also occur, and include ataxia
Ataxia
Ataxia is a neurological sign and symptom that consists of gross lack of coordination of muscle movements. Ataxia is a non-specific clinical manifestation implying dysfunction of the parts of the nervous system that coordinate movement, such as the cerebellum...
, cortical blindness, hallucinations, psychosis
Psychosis
Psychosis means abnormal condition of the mind, and is a generic psychiatric term for a mental state often described as involving a "loss of contact with reality"...
, speech problems, and coma. Other side effects include abdominal pain
Abdominal pain
Abdominal pain can be one of the symptoms associated with transient disorders or serious disease. Making a definitive diagnosis of the cause of abdominal pain can be difficult, because many diseases can result in this symptom. Abdominal pain is a common problem...
, rigors, fever
Fever
Fever is a common medical sign characterized by an elevation of temperature above the normal range of due to an increase in the body temperature regulatory set-point. This increase in set-point triggers increased muscle tone and shivering.As a person's temperature increases, there is, in...
, malaise
Malaise
Malaise is a feeling of general discomfort or uneasiness, of being "out of sorts", often the first indication of an infection or other disease. Malaise is often defined in medicinal research as a "general feeling of being unwell"...
, asthenia, acidosis
Acidosis
Acidosis is an increased acidity in the blood and other body tissue . If not further qualified, it usually refers to acidity of the blood plasma....
, tachycardia
Tachycardia
Tachycardia comes from the Greek words tachys and kardia . Tachycardia typically refers to a heart rate that exceeds the normal range for a resting heart rate...
, vasodilatation, diarrhea
Diarrhea
Diarrhea , also spelled diarrhoea, is the condition of having three or more loose or liquid bowel movements per day. It is a common cause of death in developing countries and the second most common cause of infant deaths worldwide. The loss of fluids through diarrhea can cause dehydration and...
, vomiting
Vomiting
Vomiting is the forceful expulsion of the contents of one's stomach through the mouth and sometimes the nose...
, mouth sores, loss of appetite, dermatitis
Dermatitis
-Etymology:Dermatitis derives from Greek derma "skin" + -itis "inflammation" and genetic disorder.-Terminology:There are several different types of dermatitis. The different kinds usually have in common an allergic reaction to specific allergens. The term may describe eczema, which is also called...
, dyspnea
Dyspnea
Dyspnea , shortness of breath , or air hunger, is the subjective symptom of breathlessness.It is a normal symptom of heavy exertion but becomes pathological if it occurs in unexpected situations...
, thrombocytopenia
Thrombocytopenia
Thrombocytopenia is a relative decrease of platelets in blood.A normal human platelet count ranges from 150,000 to 450,000 platelets per microliter of blood. These limits are determined by the 2.5th lower and upper percentile, so values outside this range do not necessarily indicate disease...
, and anaemia. Therefore, patients must be in good health with normal cardiovascular, hepatic, pulmonary,and neurological function to be treated with interleukin-2.
Recently, targeted therapies such as torisel, nexavar, sutent, votrient, and bevacizumab
Bevacizumab
Bevacizumab is a drug that blocks angiogenesis, the growth of new blood vessels. It is commonly used to treat various cancers, including colorectal, lung, breast, kidney, and glioblastomas....
, have been developed, and all are now approved for the treatment of metastatic renal cell carcinoma. The three to five years up to 2009 saw dramatic improvements in treatment for those with metastatic renal cell carcinoma. However, despite these improvements in therapy, overall survival remains poor.
Currently, tumor vaccines and chemotherapeutic, biologic, and immunologic agents are being researched in the treatment of metastatic renal cell carcinoma, and some appear promising. It is not known whether or not detecting metastases earlier improves survival or response to treatment.
Adjuvant therapy in renal cell carcinoma
Adjuvent therapy is typically a secondary treatment that is administered after all visible cancer has either been surgically excised, radiated or otherwise eliminated, in order to prevent any new (metastatic) cancer growths from re-appearing. The re-appearance of cancer typically occurs after micro-cancerous cells remain in the body after the primary cancer has been removed.There is currently no established adjuvant therapy for renal cell carcinoma, although there have been a number of clinical trials exploring the effectiveness of various potential treatments.
The use of non-specific cytokines has so far been shown to be ineffective. Unlike most other cancers, renal cell carcinoma is resistant to most cytotoxic and cytostatic agents,which severely limits possible effective adjuvant therapy. Trials of "cancer vaccines", radiotherapy, chemotherapy, immunotherapy, or biologic therapies (i.e. nexavar, sutent) have been met with little success,and currently the standard of care for completely resected high-risk renal cell carcinoma is close observation with no other therapy. There does appear to be some evidence that if there cancer is incompletely resected (positive surgical margins,adrenal involvement,vena caval involvement) radiotherapy reduces the risk of invasive local disease,but data is lacking on that as well.
There have also been a number of trials of Autolymphocyte therapy (ALT) which have shown varying degrees of efficacy.
ALT is a form of outpatient adoptive immunotherapy utilizing autologous ex vivo activated T-cells accompanied by high dose cimetidine.
History
Historically, RCC was also known as nephrocellular carcinoma.Paul Grawitz
Paul Grawitz
Paul Albert Grawitz was a German pathologist. While he studied medicine at the University of Berlin, he was an assistant to pathologist Rudolf Ludwig Karl Virchow . After graduation he continued as assistant to Virchow until 1886...
first described renal cell carcinoma in 1883.
See also
- Stauffer syndromeStauffer syndromeStauffer syndrome was described initially by Maurice H. Stauffer, M.D., a gastroenterologist at the Mayo Clinic in Rochester, MN. This condition is a constellation of signs and symptoms of liver dysfunction that arise due to presence of renal cell carcinoma, and, more rarely, in connection with...
- Knudson hypothesisKnudson hypothesisThe Knudson hypothesis is the hypothesis that cancer is the result of accumulated mutations to a cell's DNA. It was first proposed by Carl O. Nordling in 1953, and later formulated by Alfred G. Knudson in 1971. Knudson's work led indirectly to the identification of cancer-related genes...
- interleukin-2
- kidney cancerKidney cancerKidney cancer is a type of cancer that starts in the cells in the kidney.The two most common types of kidney cancer are renal cell carcinoma and urothelial cell carcinoma of the renal pelvis...
- rapamycin
- vinblastineVinblastineVinblastine is an antimicrotubule drug used to treat certain kinds of cancer, including Hodgkin's lymphoma, non-small cell lung cancer, breast cancer, head and neck cancer, and testicular cancer. It is also used to treat Langerhan cell histiocytosis....
- dysuriaDysuriaIn medicine, specifically urology, dysuria refers to painful urination.Difficult urination is also sometimes described as dysuria.It is one of a constellation of irritative bladder symptoms, which includes urinary frequency and haematuria....
- interferonInterferonInterferons are proteins made and released by host cells in response to the presence of pathogens—such as viruses, bacteria, or parasites—or tumor cells. They allow communication between cells to trigger the protective defenses of the immune system that eradicate pathogens or tumors.IFNs belong to...