
Gastroesophageal reflux disease
Overview
Stomach
The stomach is a muscular, hollow, dilated part of the alimentary canal which functions as an important organ of the digestive tract in some animals, including vertebrates, echinoderms, insects , and molluscs. It is involved in the second phase of digestion, following mastication .The stomach is...
into the esophagus
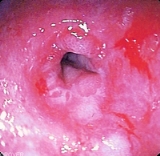
Esophagus
The esophagus is an organ in vertebrates which consists of a muscular tube through which food passes from the pharynx to the stomach. During swallowing, food passes from the mouth through the pharynx into the esophagus and travels via peristalsis to the stomach...
. A typical symptom is heartburn
Heartburn
Heartburn, also known as pyrosis or acid indigestion is a burning sensation in the chest, just behind the breastbone or in the epigastrium...
.
GERD is usually caused by changes in the barrier between the stomach
Stomach
The stomach is a muscular, hollow, dilated part of the alimentary canal which functions as an important organ of the digestive tract in some animals, including vertebrates, echinoderms, insects , and molluscs. It is involved in the second phase of digestion, following mastication .The stomach is...
and the esophagus, including abnormal relaxation of the lower esophageal sphincter, which normally holds the top of the stomach closed; impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia.
Unanswered Questions