
Botulinum toxin
Overview
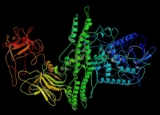
Botulinum toxin is a protein
produced by the bacterium Clostridium botulinum
, and is considered the most powerful neurotoxin
ever discovered. Botulinum toxin causes Botulism
poisoning, a serious and life-threatening illness in humans and animals. When introduced intravenously in monkeys, type A (Botox Cosmetic) of the toxin exhibits an LD50 of 40-56 ng, type C1 around 32 ng, type D 3200 ng, and type E 88 ng, rendering the above types some of the most powerful neurotoxins known.
Protein
Proteins are biochemical compounds consisting of one or more polypeptides typically folded into a globular or fibrous form, facilitating a biological function. A polypeptide is a single linear polymer chain of amino acids bonded together by peptide bonds between the carboxyl and amino groups of...
produced by the bacterium Clostridium botulinum
Clostridium botulinum
Clostridium botulinum is a Gram-positive, rod-shaped bacterium that produces several toxins. The best known are its neurotoxins, subdivided in types A-G, that cause the flaccid muscular paralysis seen in botulism. It is also the main paralytic agent in botox. C. botulinum is an anaerobic...
, and is considered the most powerful neurotoxin
Neurotoxin
A neurotoxin is a toxin that acts specifically on nerve cells , usually by interacting with membrane proteins such as ion channels. Some sources are more general, and define the effect of neurotoxins as occurring at nerve tissue...
ever discovered. Botulinum toxin causes Botulism
Botulism
Botulism also known as botulinus intoxication is a rare but serious paralytic illness caused by botulinum toxin which is metabolic waste produced under anaerobic conditions by the bacterium Clostridium botulinum, and affecting a wide range of mammals, birds and fish...
poisoning, a serious and life-threatening illness in humans and animals. When introduced intravenously in monkeys, type A (Botox Cosmetic) of the toxin exhibits an LD50 of 40-56 ng, type C1 around 32 ng, type D 3200 ng, and type E 88 ng, rendering the above types some of the most powerful neurotoxins known.