

Vitamin D
Encyclopedia

Prohormone
A prohormone is a substance that is a precursor to a hormone, usually having minimal hormonal effect by itself. The term has been used in medical science since the middle of the 20th century. The primary function of a prohormone is to enhance the strength of the hormone that already occurs in the...
and because the body can synthesize it (as vitamin D3) when sun exposure is adequate (hence its nickname, the "sunshine vitamin").
Measures of serum
Blood serum
In blood, the serum is the component that is neither a blood cell nor a clotting factor; it is the blood plasma with the fibrinogens removed...
levels (from a vitamin D3 blood test) reflect endogenous synthesis from exposure to sunlight
Sunlight
Sunlight, in the broad sense, is the total frequency spectrum of electromagnetic radiation given off by the Sun. On Earth, sunlight is filtered through the Earth's atmosphere, and solar radiation is obvious as daylight when the Sun is above the horizon.When the direct solar radiation is not blocked...
as well as intake from the diet, and it is believed that synthesis may contribute generally to the maintenance of adequate serum concentrations. The evidence indicates that the synthesis of vitamin D from sun exposure works in a feedback loop that prevents toxicity but, because of uncertainty about the cancer risk from sunlight, no recommendations are issued by the Institute of Medicine
Institute of Medicine
The Institute of Medicine is a not-for-profit, non-governmental American organization founded in 1970, under the congressional charter of the National Academy of Sciences...
for the amount of sun exposure required to meet vitamin D requirements. Accordingly, the Dietary Reference Intake
Dietary Reference Intake
The Dietary Reference Intake is a system of nutrition recommendations from the Institute of Medicine of the U.S. National Academy of Sciences. The DRI system is used by both the United States and Canada and is intended for the general public and health professionals...
s for vitamin D assume that no synthesis occurs and that all of a person's vitamin D is from their diet.
When synthesized in the kidneys, calcitriol
Calcitriol
Calcitriol , also called 1,25-dihydroxycholecalciferol or 1,25-dihydroxyvitamin D3, is the hormonally active form of vitamin D with three hydroxyl groups...
circulates as a hormone
Hormone
A hormone is a chemical released by a cell or a gland in one part of the body that sends out messages that affect cells in other parts of the organism. Only a small amount of hormone is required to alter cell metabolism. In essence, it is a chemical messenger that transports a signal from one...
, regulating the concentration of calcium
Calcium
Calcium is the chemical element with the symbol Ca and atomic number 20. It has an atomic mass of 40.078 amu. Calcium is a soft gray alkaline earth metal, and is the fifth-most-abundant element by mass in the Earth's crust...
and phosphate
Phosphate
A phosphate, an inorganic chemical, is a salt of phosphoric acid. In organic chemistry, a phosphate, or organophosphate, is an ester of phosphoric acid. Organic phosphates are important in biochemistry and biogeochemistry or ecology. Inorganic phosphates are mined to obtain phosphorus for use in...
in the bloodstream and promoting the healthy growth and remodeling of bone. Vitamin D prevents rickets
Rickets
Rickets is a softening of bones in children due to deficiency or impaired metabolism of vitamin D, magnesium , phosphorus or calcium, potentially leading to fractures and deformity. Rickets is among the most frequent childhood diseases in many developing countries...
in children and osteomalacia
Osteomalacia
Osteomalacia is the softening of the bones caused by defective bone mineralization secondary to inadequate amounts of available phosphorus and calcium, or because of overactive resorption of calcium from the bone as a result of hyperparathyroidism...
in adults, and, together with calcium, helps to protect older adults from osteoporosis
Osteoporosis
Osteoporosis is a disease of bones that leads to an increased risk of fracture. In osteoporosis the bone mineral density is reduced, bone microarchitecture is deteriorating, and the amount and variety of proteins in bone is altered...
. Vitamin D also affects neuromuscular function, inflammation
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
, and influences the action of many genes that regulate the proliferation, differentiation and apoptosis
Apoptosis
Apoptosis is the process of programmed cell death that may occur in multicellular organisms. Biochemical events lead to characteristic cell changes and death. These changes include blebbing, cell shrinkage, nuclear fragmentation, chromatin condensation, and chromosomal DNA fragmentation...
of cells.
The evidence for the health effects of vitamin D supplementation in the general population is inconsistent. The best evidence of benefit is for bone health and a decrease in mortality in elderly women.
Forms
| Name | Chemical composition | Structure |
|---|---|---|
| Vitamin D1 | molecular compound of ergocalciferol Ergocalciferol Ergocalciferol is a form of vitamin D, also called vitamin D2. It is marketed under various names including Deltalin , Drisdol and Calcidol... with lumisterol Lumisterol Lumisterol is a compound that is part of the vitamin D family of steroid compounds. It is the stereoisomer of ergosterol and was produced as a photochemical by-product in the preparation of vitamin D1, which was a mixture of vitamin D2 and lumisterol. Vitamin D2 can be formed from lumisterol by a... , 1:1 |
|
| Vitamin D2 | ergocalciferol Ergocalciferol Ergocalciferol is a form of vitamin D, also called vitamin D2. It is marketed under various names including Deltalin , Drisdol and Calcidol... (made from ergosterol Ergosterol Ergosterol is a sterol found in fungi, and named for ergot, a common name for the members of the fungal genus Claviceps from which ergosterol was first isolated. Ergosterol does not occur in plant or animal cells... ) |
 |
| Vitamin D3 | cholecalciferol Cholecalciferol Cholecalciferol is a form of vitamin D, also called vitamin D3 or calciol.It is structurally similar to steroids such as testosterone, cholesterol, and cortisol .-Forms:Vitamin D3 has several forms:... (made from 7-dehydrocholesterol 7-Dehydrocholesterol 7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun... in the skin). |
 |
| Vitamin D4 | 22-dihydroergocalciferol 22-Dihydroergocalciferol 22-Dihydroergocalciferol is a form of vitamin D, also known as vitamin D4. It has the systematic name --9,10-seco-5,7,10-ergostatrien-3-ol.-See also:*Forms of vitamin D, the five known forms of vitamin D... |
 |
| Vitamin D5 | sitocalciferol (made from 7-dehydrositosterol 7-Dehydrositosterol 7-Dehydrositosterol is a sterol which serves as a precursor for sitocalciferol .... ) |
 |
Several forms (vitamer
Vitamer
A vitamer of a particular vitamin is any of a number of chemical substances, each of which shows vitamin activity. Very commonly each "vitamin" is not a single chemical, but rather multiple chemical substances called vitamers, each of which is defined by its different biological activity.For...
s) of vitamin D exist (see table). The two major forms are vitamin D2 or ergocalciferol
Ergocalciferol
Ergocalciferol is a form of vitamin D, also called vitamin D2. It is marketed under various names including Deltalin , Drisdol and Calcidol...
, and vitamin D3 or cholecalciferol
Cholecalciferol
Cholecalciferol is a form of vitamin D, also called vitamin D3 or calciol.It is structurally similar to steroids such as testosterone, cholesterol, and cortisol .-Forms:Vitamin D3 has several forms:...
, vitamin D without a subscript refers to either D2 or D3 or both. These are known collectively as calciferol. Vitamin D2 was chemically characterized in 1932. In 1936, the chemical structure
Chemical structure
A chemical structure includes molecular geometry, electronic structure and crystal structure of molecules. Molecular geometry refers to the spatial arrangement of atoms in a molecule and the chemical bonds that hold the atoms together. Molecular geometry can range from the very simple, such as...
of vitamin D3 was established and resulted from the ultraviolet irradiation
Ultraviolet
Ultraviolet light is electromagnetic radiation with a wavelength shorter than that of visible light, but longer than X-rays, in the range 10 nm to 400 nm, and energies from 3 eV to 124 eV...
of 7-dehydrocholesterol.
Chemically, the various forms of vitamin D are secosteroids; i.e., steroid
Steroid
A steroid is a type of organic compound that contains a characteristic arrangement of four cycloalkane rings that are joined to each other. Examples of steroids include the dietary fat cholesterol, the sex hormones estradiol and testosterone, and the anti-inflammatory drug dexamethasone.The core...
s in which one of the bonds in the steroid rings is broken. The structural difference between vitamin D2 and vitamin D3 is in their side chain
Side chain
In organic chemistry and biochemistry, a side chain is a chemical group that is attached to a core part of the molecule called "main chain" or backbone. The placeholder R is often used as a generic placeholder for alkyl group side chains in chemical structure diagrams. To indicate other non-carbon...
s. The side chain of D2 contains a double bond
Double bond
A double bond in chemistry is a chemical bond between two chemical elements involving four bonding electrons instead of the usual two. The most common double bond, that between two carbon atoms, can be found in alkenes. Many types of double bonds between two different elements exist, for example in...
between carbons 22 and 23, and a methyl group
Methyl group
Methyl group is a functional group derived from methane, containing one carbon atom bonded to three hydrogen atoms —CH3. The group is often abbreviated Me. Such hydrocarbon groups occur in many organic compounds. The methyl group can be found in three forms: anion, cation and radical. The anion...
on carbon 24.
Vitamin D3 (cholecalciferol) is produced by ultraviolet irradiation
Ultraviolet
Ultraviolet light is electromagnetic radiation with a wavelength shorter than that of visible light, but longer than X-rays, in the range 10 nm to 400 nm, and energies from 3 eV to 124 eV...
(UV) of its precursor 7-dehydrocholesterol
7-Dehydrocholesterol
7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun...
. This molecule occurs naturally in the skin of animals and in milk. Vitamin D3 can be made by exposure of the skin to UV, or by exposing milk directly to UV (one commercial method).
Vitamin D2 is a derivative of ergosterol
Ergosterol
Ergosterol is a sterol found in fungi, and named for ergot, a common name for the members of the fungal genus Claviceps from which ergosterol was first isolated. Ergosterol does not occur in plant or animal cells...
, a membrane sterol
Sterol
Sterols, also known as steroid alcohols, are a subgroup of the steroids and an important class of organic molecules. They occur naturally in plants, animals, and fungi, with the most familiar type of animal sterol being cholesterol...
named for the ergot
Ergot
Ergot or ergot fungi refers to a group of fungi of the genus Claviceps. The most prominent member of this group is Claviceps purpurea. This fungus grows on rye and related plants, and produces alkaloids that can cause ergotism in humans and other mammals who consume grains contaminated with its...
fungus, which is produced by some organisms of phytoplankton
Phytoplankton
Phytoplankton are the autotrophic component of the plankton community. The name comes from the Greek words φυτόν , meaning "plant", and πλαγκτός , meaning "wanderer" or "drifter". Most phytoplankton are too small to be individually seen with the unaided eye...
, invertebrate
Invertebrate
An invertebrate is an animal without a backbone. The group includes 97% of all animal species – all animals except those in the chordate subphylum Vertebrata .Invertebrates form a paraphyletic group...
s, and fungi. The vitamin ergocalciferol
Ergocalciferol
Ergocalciferol is a form of vitamin D, also called vitamin D2. It is marketed under various names including Deltalin , Drisdol and Calcidol...
(D2) is produced in these organisms from ergosterol in response to UV irradiation. D2 is not produced by land plants or vertebrate
Vertebrate
Vertebrates are animals that are members of the subphylum Vertebrata . Vertebrates are the largest group of chordates, with currently about 58,000 species described. Vertebrates include the jawless fishes, bony fishes, sharks and rays, amphibians, reptiles, mammals, and birds...
s, because they lack the precursor ergosterol. The biological fate for producing 25(OH)D from vitamin D2 is expected to be the same as for D3, although some controversy exists over whether or not D2 can fully substitute for vitamin D3 in the human diet.
Evolution
The photosynthesis of vitamin D evolved over an estimated 750 million years ago; the phytoplankton coccolithophoreCoccolithophore
Coccolithophores are single-celled algae, protists, and phytoplankton belonging to the division of haptophytes. They are distinguished by special calcium carbonate plates of uncertain function called coccoliths , which are important microfossils...
Emiliania huxleyi
Emiliania huxleyi
Emiliania huxleyi, often abbreviated "EHUX", is a species of coccolithophore with a global distribution from the tropics to subarctic waters. It is one of thousands of different photosynthetic plankton that freely drift in the euphotic zone of the ocean, forming the basis of virtually all marine...
is an early example. Vitamin D played a critical role in the maintenance of a calcified skeleton in vertebrates as they left their calcium-rich ocean environment for land over an estimated 350 million years ago.
Vitamin D can be synthesized only via a photochemical process, so early vertebrates that ventured onto land either had to ingest foods that contained vitamin D or had to be exposed to sunlight to photosynthesize vitamin D in their skin to satisfy their body's vitamin D requirement.
Production in the skin
7-Dehydrocholesterol
7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun...
reacts with ultraviolet light (UVB) at wavelengths between 270 and 300 nm, with peak synthesis occurring between 295 and 297 nm. These wavelengths are present in sunlight when the UV index
UV index
The ultraviolet index or UV Index is an international standard measurement of the strength of the ultraviolet radiation from the sun at a particular place on a particular day...
is greater than three, as well as in the light emitted by the UV lamps in tanning beds (which produce ultraviolet primarily in the UVA spectrum, but typically produce 4% to 10% of the total UV emissions as UVB). At a UV index greater than three, which occurs daily within the tropics
Tropics
The tropics is a region of the Earth surrounding the Equator. It is limited in latitude by the Tropic of Cancer in the northern hemisphere at approximately N and the Tropic of Capricorn in the southern hemisphere at S; these latitudes correspond to the axial tilt of the Earth...
, daily during the spring and summer seasons in temperate regions, and almost never within the arctic circle
Arctic Circle
The Arctic Circle is one of the five major circles of latitude that mark maps of the Earth. For Epoch 2011, it is the parallel of latitude that runs north of the Equator....
s, vitamin D3 can be made in the skin. Latitude does not consistently predict the average serum 25OHD level of a population. The assumption that vitamin D levels in the population follow a latitude gradient is especially questionable in view of surveys which have shown that UVB penetrating to the earth's surface over 24 hours during the summer months in northern Canada equals or exceeds UVB penetration at the equator. Accordingly, there is sufficient opportunity during the spring, summer, and fall months at high latitude for humans to form and store vitamin D3.
Depending on the intensity of UVB rays and the minutes of exposure, an equilibrium can develop in the skin, and vitamin D degrades as fast as it is generated.
The skin consists of two primary layers: the inner layer called the dermis
Dermis
The dermis is a layer of skin between the epidermis and subcutaneous tissues, and is composed of two layers, the papillary and reticular dermis...
, composed largely of connective tissue
Connective tissue
"Connective tissue" is a fibrous tissue. It is one of the four traditional classes of tissues . Connective Tissue is found throughout the body.In fact the whole framework of the skeleton and the different specialized connective tissues from the crown of the head to the toes determine the form of...
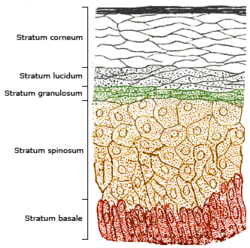
, and the outer, thinner epidermis. Thick epidermis in the soles and palms consists of five strata; from outer to inner they are: the stratum corneum
Stratum corneum
The stratum corneum is the outermost layer of the epidermis, consisting of dead cells that lack nuclei and organelles. The purpose of the stratum corneum is to form a barrier to protect underlying tissue from infection, dehydration, chemicals and mechanical stress...
, stratum lucidum
Stratum lucidum
The stratum lucidum is a thin, clear layer of dead skin cells in the epidermis named for its translucent appearance under a microscope...
, stratum granulosum
Stratum granulosum
The stratum granulosum is a thin layer of cells in the epidermis. Keratinocytes migrating from the underlying stratum spinosum become known as granular cells in this layer...
, stratum spinosum
Stratum spinosum
The stratum spinosum is a layer of the epidermis found between the stratum granulosum and stratum basale. This layer is also referred to as the "spinous" or "prickle-cell" layer. This appearance is due to desmosomal connections of adjacent cells. Keratinization begins in the stratum spinosum....
, and stratum basale. Vitamin D is produced in the two innermost strata, the stratum basale and stratum spinosum.
Cholecalciferol is produced photochemically in the skin
Skin
-Dermis:The dermis is the layer of skin beneath the epidermis that consists of connective tissue and cushions the body from stress and strain. The dermis is tightly connected to the epidermis by a basement membrane. It also harbors many Mechanoreceptors that provide the sense of touch and heat...
from 7-dehydrocholesterol
7-Dehydrocholesterol
7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun...
; 7-dehydrocholesterol is produced in relatively large quantities in the skin of most vertebrate animals, including humans. The naked mole rat
Naked Mole Rat
The naked mole rat , also known as the sand puppy or desert mole rat, is a burrowing rodent native to parts of East Africa and the only species currently classified in the genus Heterocephalus...
appears to be naturally cholecalciferol deficient, as serum 25-OH vitamin D levels are undetectable.
In some animals, the presence of fur or feathers blocks the UV rays from reaching the skin. In birds and fur-bearing mammals, vitamin D is generated from the oily secretions of the skin deposited onto the feathers or fur and is obtained orally during grooming.
History
American researchers Elmer McCollumElmer McCollum
Elmer Verner McCollum was an American biochemist known for his work on the influence of diet on health.-Life and education:McCollum was born on a farm near Fort Scott, Kansas, where he spent his first seventeen years...
and Marguerite Davis
Marguerite Davis
Marguerite Davis was the co-discoverer of Vitamin A and Vitamin B with Elmer Verner McCollum in 1913..-External links:*...
in 1913 discovered a substance in cod liver oil
Cod liver oil
Cod liver oil is a nutritional supplement derived from liver of cod fish. It has high levels of the omega-3 fatty acids, EPA and DHA, and very high levels of vitamin A and vitamin D. It is widely taken to ease the symptoms of arthritis and for other health benefits...
which later was called "vitamin A". British doctor Edward Mellanby noticed dogs that were fed cod liver oil did not develop rickets and concluded vitamin A, or a closely associated factor, could prevent the disease. In 1921, Elmer McCollum tested modified cod liver oil in which the vitamin A had been destroyed. The modified oil cured the sick dogs, so McCollum concluded the factor in cod liver oil which cured rickets was distinct from vitamin A. He called it vitamin D because it was the fourth vitamin to be named. It was not initially realized that, unlike other vitamins, vitamin D can be synthesised by humans through exposure to UV light.
In 1923, it was established that when 7-dehydrocholesterol
7-Dehydrocholesterol
7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun...
is irradiated with light, a form of a fat-soluble vitamin is produced (now known as D3). Alfred Fabian Hess
Alfred Fabian Hess
Alfred Fabian Hess was an American physician known for his work on the role of nutrition in scurvy and rickets and for describing the Hess test.- Biography :...
showed "light equals vitamin D." Adolf Windaus
Adolf Otto Reinhold Windaus
Adolf Otto Reinhold Windaus was a German chemist who won a Nobel Prize in Chemistry in 1928 for his work on sterols and their relation to vitamins. He was the doctoral advisor of Adolf Butenandt who also won a Nobel Prize in Chemistry in 1939.Adolf Windaus was born in Berlin. His interest in...
, at the University of Göttingen in Germany, received the Nobel Prize in Chemistry
Nobel Prize in Chemistry
The Nobel Prize in Chemistry is awarded annually by the Royal Swedish Academy of Sciences to scientists in the various fields of chemistry. It is one of the five Nobel Prizes established by the will of Alfred Nobel in 1895, awarded for outstanding contributions in chemistry, physics, literature,...
in 1928, for his work on the constitution of sterol
Sterol
Sterols, also known as steroid alcohols, are a subgroup of the steroids and an important class of organic molecules. They occur naturally in plants, animals, and fungi, with the most familiar type of animal sterol being cholesterol...
s and their connection with vitamins. In the 1930s he clarified further the chemical structure of vitamin D.
In 1923, Harry Steenbock
Harry Steenbock
Harry Steenbock was a Professor of Biochemistry at the University of Wisconsin–Madison.-Vitamin D:...
at the University of Wisconsin demonstrated that irradiation by ultraviolet light increased the vitamin D content of foods and other organic materials.After irradiating rodent food, Steenbock discovered the rodents were cured of rickets. A vitamin D deficiency is a known cause of rickets. Using $300 of his own money, Steenbock patented his invention. His irradiation technique was used for foodstuffs, most memorably for milk. By the expiration of his patent in 1945, rickets had been all but eliminated in the US.
Mechanism of action
Vitamin D is carried in the bloodstream to the liver, where it is converted into the prohormoneProhormone
A prohormone is a substance that is a precursor to a hormone, usually having minimal hormonal effect by itself. The term has been used in medical science since the middle of the 20th century. The primary function of a prohormone is to enhance the strength of the hormone that already occurs in the...
calcidiol
Calcidiol
Calcifediol , also known as calcidiol, 25-hydroxycholecalciferol, or 25-hydroxyvitamin D , is a prehormone that is produced in the liver by hydroxylation of vitamin D3 by the enzyme cholecalciferol 25-hydroxylase...
. Circulating calcidiol may then be converted into calcitriol
Calcitriol
Calcitriol , also called 1,25-dihydroxycholecalciferol or 1,25-dihydroxyvitamin D3, is the hormonally active form of vitamin D with three hydroxyl groups...
, the biologically active form of vitamin D, either in the kidneys or by monocyte
Monocyte
Monocytes are a type of white blood cell and are part of the innate immune system of vertebrates including all mammals , birds, reptiles, and fish. Monocytes play multiple roles in immune function...
-macrophages in the immune system
Immune system
An immune system is a system of biological structures and processes within an organism that protects against disease by identifying and killing pathogens and tumor cells. It detects a wide variety of agents, from viruses to parasitic worms, and needs to distinguish them from the organism's own...
. When synthesized by monocyte-macrophages, calcitriol acts locally as a cytokine
Cytokine
Cytokines are small cell-signaling protein molecules that are secreted by the glial cells of the nervous system and by numerous cells of the immune system and are a category of signaling molecules used extensively in intercellular communication...
, defending the body against microbial invaders.
Following the final converting step in the kidney, calcitriol (the physiologically active form of vitamin D) is released into the circulation. By binding to vitamin D-binding protein (VDBP), a carrier protein in the plasma
Blood plasma
Blood plasma is the straw-colored liquid component of blood in which the blood cells in whole blood are normally suspended. It makes up about 55% of the total blood volume. It is the intravascular fluid part of extracellular fluid...
, calcitriol is transported to various target organs.
Calcitriol mediates its biological effects by binding to the vitamin D receptor (VDR), which is principally located in the nuclei
Cell nucleus
In cell biology, the nucleus is a membrane-enclosed organelle found in eukaryotic cells. It contains most of the cell's genetic material, organized as multiple long linear DNA molecules in complex with a large variety of proteins, such as histones, to form chromosomes. The genes within these...
of target cells. The binding of calcitriol to the VDR allows the VDR to act as a transcription factor
Transcription factor
In molecular biology and genetics, a transcription factor is a protein that binds to specific DNA sequences, thereby controlling the flow of genetic information from DNA to mRNA...
that modulates the gene expression
Gene expression
Gene expression is the process by which information from a gene is used in the synthesis of a functional gene product. These products are often proteins, but in non-protein coding genes such as ribosomal RNA , transfer RNA or small nuclear RNA genes, the product is a functional RNA...
of transport proteins (such as TRPV6
TRPV6
TRPV6 is a membrane calcium channel which is responsible for the first step in calcium absorption in the intestine. It was first named CAT1, or ECaC2, and has been described in the intestine in several species, including humans. It is located in the apical brush-border membrane of the intestinal...
and calbindin
Calbindin
Calbindin refers to several calcium-binding proteins. They were originally described as vitamin D-dependent calcium-binding proteins in the intestine and kidney in the chick and mammals...
), which are involved in calcium absorption in the intestine.
The vitamin D receptor belongs to the nuclear receptor
Nuclear receptor
In the field of molecular biology, nuclear receptors are a class of proteins found within cells that are responsible for sensing steroid and thyroid hormones and certain other molecules...
superfamily of steroid/thyroid hormone receptors
Steroid hormone receptor
Steroid hormone receptors are found on the plasma membrane, in the cytosol and also in the nucleus of target cells. They are generally intracellular receptors and initiate signal transduction for steroid hormones which lead to changes in gene expression over a time period of hours to days...
, and VDRs are expressed by cells in most organs, including the brain
Brain
The brain is the center of the nervous system in all vertebrate and most invertebrate animals—only a few primitive invertebrates such as sponges, jellyfish, sea squirts and starfishes do not have one. It is located in the head, usually close to primary sensory apparatus such as vision, hearing,...
, heart
Heart
The heart is a myogenic muscular organ found in all animals with a circulatory system , that is responsible for pumping blood throughout the blood vessels by repeated, rhythmic contractions...
, skin, gonads, prostate
Prostate
The prostate is a compound tubuloalveolar exocrine gland of the male reproductive system in most mammals....
, and breast
Breast
The breast is the upper ventral region of the torso of a primate, in left and right sides, which in a female contains the mammary gland that secretes milk used to feed infants.Both men and women develop breasts from the same embryological tissues...
. VDR activation in the intestine, bone, kidney, and parathyroid gland cells leads to the maintenance of calcium
Calcium
Calcium is the chemical element with the symbol Ca and atomic number 20. It has an atomic mass of 40.078 amu. Calcium is a soft gray alkaline earth metal, and is the fifth-most-abundant element by mass in the Earth's crust...
and phosphorus
Phosphorus
Phosphorus is the chemical element that has the symbol P and atomic number 15. A multivalent nonmetal of the nitrogen group, phosphorus as a mineral is almost always present in its maximally oxidized state, as inorganic phosphate rocks...
levels in the blood
Blood
Blood is a specialized bodily fluid in animals that delivers necessary substances such as nutrients and oxygen to the cells and transports metabolic waste products away from those same cells....
(with the assistance of parathyroid hormone and calcitonin
Calcitonin
Calcitonin is a 32-amino acid linear polypeptide hormone that is producedin humans primarily by the parafollicular cells of the thyroid, and in many other animals in the ultimobranchial body. It acts to reduce blood calcium , opposing the effects of parathyroid hormone . Calcitonin has been found...
) and to the maintenance of bone
Bone
Bones are rigid organs that constitute part of the endoskeleton of vertebrates. They support, and protect the various organs of the body, produce red and white blood cells and store minerals. Bone tissue is a type of dense connective tissue...
content.
Vitamin D increases expression of the tyrosine hydroxylase
Tyrosine hydroxylase
Tyrosine hydroxylase or tyrosine 3-monooxygenase is the enzyme responsible for catalyzing the conversion of the amino acid L-tyrosine to dihydroxyphenylalanine . It does so using tetrahydrobiopterin as a coenzyme. DOPA is a precursor for dopamine, which, in turn, is a precursor for norepinephrine ...
gene in adrenal medullary cells. It also is involved in the biosynthesis of neurotrophic factors, synthesis of nitric oxide synthase, and increased glutathione levels.
The VDR is known to be involved in cell proliferation and differentiation
Cellular differentiation
In developmental biology, cellular differentiation is the process by which a less specialized cell becomes a more specialized cell type. Differentiation occurs numerous times during the development of a multicellular organism as the organism changes from a simple zygote to a complex system of...
. Vitamin D also affects the immune system, and VDRs are expressed in several white blood cell
White blood cell
White blood cells, or leukocytes , are cells of the immune system involved in defending the body against both infectious disease and foreign materials. Five different and diverse types of leukocytes exist, but they are all produced and derived from a multipotent cell in the bone marrow known as a...
s, including monocytes and activated T
T cell
T cells or T lymphocytes belong to a group of white blood cells known as lymphocytes, and play a central role in cell-mediated immunity. They can be distinguished from other lymphocytes, such as B cells and natural killer cells , by the presence of a T cell receptor on the cell surface. They are...
and B cell
B cell
B cells are lymphocytes that play a large role in the humoral immune response . The principal functions of B cells are to make antibodies against antigens, perform the role of antigen-presenting cells and eventually develop into memory B cells after activation by antigen interaction...
s.
Apart from VDR activation, various alternative mechanisms of action are known. An important one of these is its role as a natural inhibitor of signal transduction by hedgehog
Hedgehog signaling pathway
In a growing embryo, cells develop differently in the head or tail end of the embryo, the left or right, and other positions. They also form segments which develop into different body parts. The hedgehog signaling pathway gives cells information that they need to make the embryo develop properly....
(a hormone involved in morphogenesis).
One of the most important roles of vitamin D is to maintain skeletal calcium balance by promoting calcium absorption
Calcium metabolism
Calcium metabolism or calcium homeostasis is the mechanism by which the body maintains adequate calcium levels. Derangements of this mechanism lead to hypercalcemia or hypocalcemia, both of which can have important consequences for health....
in the intestines, promoting bone resorption
Bone resorption
Bone resorption is the process by which osteoclasts break down bone and release the minerals, resulting in a transfer of calcium from bone fluid to the blood....
by increasing osteoclast
Osteoclast
An osteoclast is a type of bone cell that removes bone tissue by removing its mineralized matrix and breaking up the organic bone . This process is known as bone resorption. Osteoclasts were discovered by Kolliker in 1873...
number, maintaining calcium and phosphate
Phosphate
A phosphate, an inorganic chemical, is a salt of phosphoric acid. In organic chemistry, a phosphate, or organophosphate, is an ester of phosphoric acid. Organic phosphates are important in biochemistry and biogeochemistry or ecology. Inorganic phosphates are mined to obtain phosphorus for use in...
levels for bone formation, and allowing proper functioning of parathyroid hormone
Parathyroid hormone
Parathyroid hormone , parathormone or parathyrin, is secreted by the chief cells of the parathyroid glands as a polypeptide containing 84 amino acids...
to maintain serum calcium levels. Vitamin D deficiency can result in lower bone mineral density and an increased risk of bone loss (osteoporosis
Osteoporosis
Osteoporosis is a disease of bones that leads to an increased risk of fracture. In osteoporosis the bone mineral density is reduced, bone microarchitecture is deteriorating, and the amount and variety of proteins in bone is altered...
) or bone fracture because a lack of vitamin D alters mineral metabolism in the body.
Health effects
The effects of vitamin D supplementation on health is uncertain. A United States Institute of MedicineInstitute of Medicine
The Institute of Medicine is a not-for-profit, non-governmental American organization founded in 1970, under the congressional charter of the National Academy of Sciences...
(IOM) report states: "Outcomes related to cancer
Cancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
/neoplasms, cardiovascular disease
Cardiovascular disease
Heart disease or cardiovascular disease are the class of diseases that involve the heart or blood vessels . While the term technically refers to any disease that affects the cardiovascular system , it is usually used to refer to those related to atherosclerosis...
and hypertension
Hypertension
Hypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
, diabetes and metabolic syndrome, falls and physical performance, immune functioning and autoimmune disorders, infections, neuropsychological functioning, and preeclampsia could not be linked reliably with calcium or vitamin D intake and were often conflicting." Some researchers claim the IOM was too definitive in its recommendations and made a mathematical mistake when calculating the blood level of vitamin D associated with bone health. Members of the IOM panel maintain that they used a "standard procedure for dietary recommendations" and that the report is solidly based on the data. Research on vitamin D supplements, including large scale clinical trials, is continuing.
Mortality
Low blood levels of vitamin D are associated with increased mortality. Supplemental vitamin D3 appears to decrease all cause mortality, with the best evidence of a benefit in elderly women. Vitamin D2, alfacalcidol, and calcitriol do not appear to be effective.Overall, excess or deficiency in the calciferol system appear to cause abnormal functioning and premature aging. The data suggest a U-shaped risk curve between serum 25OHD level and all-cause mortality with an increased risk at low and high serum levels. The detrimental effects appear at a lower level in people with black skin.
Bone health
Low serum vitamin D levels are associated with ricketsRickets
Rickets is a softening of bones in children due to deficiency or impaired metabolism of vitamin D, magnesium , phosphorus or calcium, potentially leading to fractures and deformity. Rickets is among the most frequent childhood diseases in many developing countries...
, fall
Falling (accident)
Falling is a major cause of personal injury, especially for the elderly. Builders, electricians, miners, and painters represent worker categories representing high rates of fall injuries. The WHO estimate that 392,000 people die in falls every year...
s, and low bone mineral density. Supplementation with vitamin D and calcium
Calcium
Calcium is the chemical element with the symbol Ca and atomic number 20. It has an atomic mass of 40.078 amu. Calcium is a soft gray alkaline earth metal, and is the fifth-most-abundant element by mass in the Earth's crust...
improves bone mineral density slightly, as well as decreases the risk falls and fractures in certain groups of people. The quality of the evidence is, however, poor.
Cardiovascular disease
Evidence for health effects from vitamin D supplementation for cardiovascular health is poor. Moderate to high doses may reduce cardiovascular disease risk but are of questionable clinical significance.Cancer
Low vitamin D levels are associated with some cancerCancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
s. When supplementation is used to treat people with prostate cancer
Prostate cancer
Prostate cancer is a form of cancer that develops in the prostate, a gland in the male reproductive system. Most prostate cancers are slow growing; however, there are cases of aggressive prostate cancers. The cancer cells may metastasize from the prostate to other parts of the body, particularly...
, however, there does not appear to be a benefit. Results for a protective or harmful effect of vitamin D supplementation in other types of cancer are inconclusive.
Tuberculosis
Historically, vitamin D3 was used to treat tuberculosis patients, but has not been adequately investigated in controlled clinical trials. The hormonally active form of vitamin D3, 1,25-dihydroxycholecalciferol (1,25(OH)2D), has been shown to have antimycobacterialAntimycobacterial
An antimycobacterial is a type of drug used to treat Mycobacteria infections.Types include:* Tuberculosis treatments* Leprostatic agents...
activity in vitro
In vitro
In vitro refers to studies in experimental biology that are conducted using components of an organism that have been isolated from their usual biological context in order to permit a more detailed or more convenient analysis than can be done with whole organisms. Colloquially, these experiments...
, but the applicability of this effect to clinical situations has not been shown.
One study found that vitamin D metabolites regulate the expression of cathelicidin
Cathelicidin
Members of the cathelicidin family of antimicrobial polypeptides are characterized by a highly conserved region and a highly variable cathelicidin peptide domain.Cathelicidin peptides have been isolated from many different species of mammals...
which is an antimicrobial peptide with activity against Mycobacterium tuberculosis, and that the prevalence of vitamin D insufficiency (serium 25(OH)D concentration < 30 ng/mL) in patients with active tuberculosis was 86%.
Nine placebo controlled, double-blind studies provided "strongest evidence" supporting "vitamin D therapy for tuberculosis, influenza, and viral upper respiratory tract illnesses."
In one study, vitamin D3 supplementations did not show any improvement in treating tuberculosis except in a small subset of patients with the tt genotype of the TaqI vitamin D receptor polymorphism.
Several studies have shown an association between low serum levels of 25-hydroxycholecalciferol (25(OH)D) and increased risk for both active tuberculosis
Tuberculosis
Tuberculosis, MTB, or TB is a common, and in many cases lethal, infectious disease caused by various strains of mycobacteria, usually Mycobacterium tuberculosis. Tuberculosis usually attacks the lungs but can also affect other parts of the body...
disease progression and susceptibility. More prospective studies will be required to ascertain the potential role of vitamin D supplementation in treating patients with tuberculosis.
Other
Vitamin D appears to have a protective effect against multiple sclerosisMultiple sclerosis
Multiple sclerosis is an inflammatory disease in which the fatty myelin sheaths around the axons of the brain and spinal cord are damaged, leading to demyelination and scarring as well as a broad spectrum of signs and symptoms...
. While the initial hypothesis was based on that fact that MS occurred at high rates in the region of the world with long periods with little sunlight further supportive evidence is now available. The relationship between latitude and UVB penetration is however complicated by factors such as atmosphere height (50% higher at the equator), cloud cover (denser at the equator) and ozone layer density, and latitude does not consistently predict the average serum vitamin D level of a population. UVB penetrating to the earth's surface over 24 hours during the summer months in northern Canada (where summer days are longer) equals or exceeds UVB penetration at the equator, allowing sufficient opportunity during the spring, summer, and fall at high latitude to form and store vitamin D3. This, combined with recent computer modeling may call into question the assumption that vitamin D levels in the population follow a latitude gradient.[] Whether vitamin D supplements during pregnancy can lessen the likelihood of the child developing MS later in life is not known.
Vitamin D appears to have effects on immune function. It has been postulated to play a role in influenza
Vitamin D and influenza
Numerous studies link vitamin D and influenza, as well as vitamin D and respiratory infections more generally. This vitamin up-regulates genetic expression of various endogenous antimicrobial peptides , which exhibit broad-spectrum microbicidal activity against bacteria, fungi, and viruses...
with lack of vitamin D synthesis during the winter as one explanation for high rates of influenza infection during the winter. For viral infections, other implicated factors include low relative humidities produced by indoor heating and cold temperatures that favor virus spread.
Deficiency
Low blood calcidiol (25-hydroxy-vitamin D) can result from avoiding the sun. Deficiency results in impaired bone mineralization, and leads to bone softening diseases including:- RicketsRicketsRickets is a softening of bones in children due to deficiency or impaired metabolism of vitamin D, magnesium , phosphorus or calcium, potentially leading to fractures and deformity. Rickets is among the most frequent childhood diseases in many developing countries...
, a childhood disease characterized by impeded growth and deformity of the long bones, can be caused by calcium or phosphorus deficiency as well as a lack of vitamin D; today it is largely found in low income countries in Africa, Asia or the Middle East and in those with genetic disorders such as pseudovitamin D deficiency rickets. Rickets was first described in 1650, by Francis GlissonFrancis GlissonFrancis Glisson was a British physician, anatomist, and writer on medical subjects. He did important work on the anatomy of the liver, and he wrote an early pediatric text on rickets...
who said it had first appeared about 30 years previously in the counties of DorsetDorsetDorset , is a county in South West England on the English Channel coast. The county town is Dorchester which is situated in the south. The Hampshire towns of Bournemouth and Christchurch joined the county with the reorganisation of local government in 1974...
and SomersetSomersetThe ceremonial and non-metropolitan county of Somerset in South West England borders Bristol and Gloucestershire to the north, Wiltshire to the east, Dorset to the south-east, and Devon to the south-west. It is partly bounded to the north and west by the Bristol Channel and the estuary of the...
. In 1857, John SnowJohn Snow (physician)John Snow was an English physician and a leader in the adoption of anaesthesia and medical hygiene. He is considered to be one of the fathers of epidemiology, because of his work in tracing the source of a cholera outbreak in Soho, England, in 1854.-Early life and education:Snow was born 15 March...
suggested the rickets then widespread in Britain was being caused by the adulteration of bakers bread with alumAlumAlum is both a specific chemical compound and a class of chemical compounds. The specific compound is the hydrated potassium aluminium sulfate with the formula KAl2.12H2O. The wider class of compounds known as alums have the related empirical formula, AB2.12H2O.-Chemical properties:Alums are...
. The role of diet in the development of rickets was determined by Edward Mellanby between 1918–1920. Nutritional rickets exists in countries with intense year round sunlight such as Nigeria and can occur without vitamin D deficiency. Although rickets and osteomalacia are now rare in Britain there have been outbreaks in some immigrant communities in which osteomalacia sufferers included women with seemingly adequate daylight outdoor exposure wearing Western clothing. Having darker skin and reduced exposure to sunshine did not produce rickets unless the diet deviated from a Western omnivore pattern characterized by high intakes of meat, fish and eggs, and low intakes of high-extraction cereals. The dietary risk factors for rickets include abstaining from animal foods. Vitamin D deficiency remains the main cause of rickets among young infants in most countries, because breast milk is low in vitamin D and social customs and climatic conditions can prevent adequate UVB exposure. In sunny countries such as Nigeria, South Africa, and Bangladesh where the disease occurs among older toddlers and children it has been attributed to low dietary calcium intakes, which are characteristic of cereal-based diets with limited access to dairy products. Rickets was formerly a major public health problem among the US population; in Denver where ultraviolet rays are approximately 20% stronger than at sea level on the same latitude almost two thirds of 500 children had mild rickets in the late 1920s. An increase in the proportion of animal protein in the 20th century American diet coupled with increased consumption of milk fortified with relatively small quantities of vitamin D coincided with a dramatic decline in the number of rickets cases. - OsteomalaciaOsteomalaciaOsteomalacia is the softening of the bones caused by defective bone mineralization secondary to inadequate amounts of available phosphorus and calcium, or because of overactive resorption of calcium from the bone as a result of hyperparathyroidism...
, a bone-thinning disorder that occurs exclusively in adults and is characterized by proximal muscle weakness and bone fragility. The effects of osteomalacia are thought to contribute to chronic musculoskeletal painPainPain is an unpleasant sensation often caused by intense or damaging stimuli such as stubbing a toe, burning a finger, putting iodine on a cut, and bumping the "funny bone."...
, there is no persuasive evidence of lower vitamin D status in chronic pain sufferers.
Adequate vitamin D may also be associated with healthy hair follicle
Hair follicle
A hair follicle is a skin organ that produces hair. Hair production occurs in phases, including a growth phase , and cessation phase , and a rest phase . Stem cells are principally responsible for the production of hair....
growth cycles. There are also associations between low 25(OH)D levels and peripheral vascular disease, certain cancer
Cancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
s, multiple sclerosis
Multiple sclerosis
Multiple sclerosis is an inflammatory disease in which the fatty myelin sheaths around the axons of the brain and spinal cord are damaged, leading to demyelination and scarring as well as a broad spectrum of signs and symptoms...
, rheumatoid arthritis
Rheumatoid arthritis
Rheumatoid arthritis is a chronic, systemic inflammatory disorder that may affect many tissues and organs, but principally attacks synovial joints. The process produces an inflammatory response of the synovium secondary to hyperplasia of synovial cells, excess synovial fluid, and the development...
, juvenile diabetes
Diabetes mellitus type 1
Diabetes mellitus type 1 is a form of diabetes mellitus that results from autoimmune destruction of insulin-producing beta cells of the pancreas. The subsequent lack of insulin leads to increased blood and urine glucose...
, Parkinson's
Parkinson's disease
Parkinson's disease is a degenerative disorder of the central nervous system...
and Alzheimer's disease
Alzheimer's disease
Alzheimer's disease also known in medical literature as Alzheimer disease is the most common form of dementia. There is no cure for the disease, which worsens as it progresses, and eventually leads to death...
. However these associations were found in observational studies
Observational study
In epidemiology and statistics, an observational study draws inferences about the possible effect of a treatment on subjects, where the assignment of subjects into a treated group versus a control group is outside the control of the investigator...
and vitamin D vitamin supplements
Multivitamin
A multivitamin is a preparation intended to supplement a human diet with vitamins, dietary minerals, and other nutritional elements. Such preparations are available in the form of tablets, capsules, pastilles, powders, liquids, and injectable formulations...
have not been demonstrated to reduce the risks of these diseases.
Research shows that dark-skinned people living in temperate climates have lower vitamin D levels. It has been suggested that dark-skinned people are less efficient at making vitamin D because melanin
Melanin
Melanin is a pigment that is ubiquitous in nature, being found in most organisms . In animals melanin pigments are derivatives of the amino acid tyrosine. The most common form of biological melanin is eumelanin, a brown-black polymer of dihydroxyindole carboxylic acids, and their reduced forms...
in the skin hinders vitamin D synthesis, however a recent study has found novel evidence that low vitamin D levels among Africans may be due to other reasons.Recent evidence implicates parathyroid hormone
Parathyroid hormone
Parathyroid hormone , parathormone or parathyrin, is secreted by the chief cells of the parathyroid glands as a polypeptide containing 84 amino acids...
in adverse cardiovascular outcomes, black women have an increase in serum PTH at a lower 25(OH)D level than white women. A large scale association study of the genetic determinants of vitamin D insufficiency in Caucasians found no links to pigmentation.
The Director General of Research and Development and Chief Scientific Adviser for the UK Department of Health and NHS said that children aged six months to five years should be given vitamin D supplements—particularly during the winter. However, people who get enough vitamin D from their diet and from sunlight are not recommended for vitamin D supplements.
With an emphasis on recommending treatment and intake levels for patients at risk of deficiency listed below, a panel of experts issued a clinical guideline in 2011, stating that vitamin D2 and D3 sources are equivalent.
Toxicity
In healthy adults, sustained intake of more than 1250 micrograms/day (50,000 IU) can produce overt toxicityToxicity
Toxicity is the degree to which a substance can damage a living or non-living organisms. Toxicity can refer to the effect on a whole organism, such as an animal, bacterium, or plant, as well as the effect on a substructure of the organism, such as a cell or an organ , such as the liver...
after several months; those with certain medical conditions such as primary hyperparathyroidism
Hyperparathyroidism
Hyperparathyroidism is overactivity of the parathyroid glands resulting in excess production of parathyroid hormone . The parathyroid hormone regulates calcium and phosphate levels and helps to maintain these levels...
are far more sensitive to vitamin D and develop hypercalcemia in response to any increase in vitamin D nutrition, while maternal hypercalcemia during pregnancy may increase fetal sensitivity to effects of vitamin D and lead to a syndrome of mental retardation and facial deformities. Pregnant or breastfeeding women should consult a doctor before taking a vitamin D supplement. For infants (birth to 12 months), the tolerable upper limit (maximum amount that can be tolerated without harm) is set at 25 micrograms/day (1000 IU). One thousand micrograms (40,000 IU) per day in infants has produced toxicity within one month. After being commissioned by the Canadian and American governments, the Institute of Medicine (IOM) , has increased the tolerable upper limit (UL) to 2500 IU per day for ages 1–3 years, 3000 IU per day for ages 4–8 years and 4000 IU per day for ages 9–71+ years (including pregnant or lactating women). Vitamin D overdose causes hypercalcemia, and the main symptoms of vitamin D overdose are those of hypercalcemia: anorexia
Anorexia (symptom)
Anorexia is the decreased sensation of appetite...
, nausea, and vomiting can occur, frequently followed by polyuria
Polyuria
Polyuria is a condition usually defined as excessive or abnormally large production or passage of urine . Frequent urination is sometimes included by definition, but is nonetheless usually an accompanying symptom...
, polydipsia
Polydipsia
Polydipsia is a medical symptom in which the patient displays excessive thirst. The word derives from the Greek πολυδιψία, which is derived from πολύς + δίψα...
, weakness, nervousness, pruritus, and, ultimately, renal failure
Renal failure
Renal failure or kidney failure describes a medical condition in which the kidneys fail to adequately filter toxins and waste products from the blood...
.Proteinuria
Proteinuria
Proteinuria means the presence of anexcess of serum proteins in the urine. The protein in the urine often causes the urine to become foamy, although foamy urine may also be caused by bilirubin in the urine , retrograde ejaculation, pneumaturia due to a fistula, or drugs such as pyridium.- Causes...
, urinary casts
Urinary casts
Urinary casts are cylindrical structures produced by the kidney and present in the urine in certain disease states. They form in the distal convoluted tubule and collecting ducts of nephrons, then dislodge and pass into the urine, where they can be detected by microscopy.They form via precipitation...
, azotemia
Azotemia
Azotemia is a medical condition characterized by abnormally high levels of nitrogen-containing compounds, such as urea, creatinine, various body waste compounds, and other nitrogen-rich compounds in the blood...
, and metastatic calcification
Metastatic calcification
Metastatic calcification is deposition of calcium salts in otherwise normal tissue, because of elevated serum levels of calcium in blood, which can occur because of deranged metabolism as well as increased absorption or decreased excretion of calcium and related minerals.It occurs as opposed to...
(especially in the kidneys) may develop. Vitamin D toxicity is treated by discontinuing vitamin D supplementation and restricting calcium intake. Kidney damage may be irreversible. Exposure to sunlight for extended periods of time does not normally cause vitamin D toxicity. Within about 20 minutes of ultraviolet exposure in light skinned individuals (3–6 times longer for pigmented skin), the concentrations of vitamin D precursors produced in the skin reach an equilibrium
Chemical equilibrium
In a chemical reaction, chemical equilibrium is the state in which the concentrations of the reactants and products have not yet changed with time. It occurs only in reversible reactions, and not in irreversible reactions. Usually, this state results when the forward reaction proceeds at the same...
, and any further vitamin D that is produced is degraded.According to some sources, endogenous production with full body exposure to sunlight is approximately 250 µg (10,000 IU) per day. According to Holick
Michael Holick
Michael Holick is an American dermatologist, a professor of medicine, physiology and biophysics at Boston University who is known for recommending exposure to sunlight 2 to 3 times per week for photosynthesis of Vitamin D. He was asked to resign from his position in dermatology at Boston...
, "the skin has a large capacity to produce cholecalciferol" his experiments indicate: "[W]hole-body exposure to one minimal erythemal dose [a dose that would just begin to produce sunburn in a given individual] of simulated solar ultraviolet radiation is comparable with taking an oral dose of between 250 and 625 micrograms (10,000 and 25,000 IU) vitamin D."
Based on the non-observation of toxicity at daily intakes of up to 50,000 IU per day, leading to calcidiol levels of more than 600 nmol/L, and the similar effect of supplementation and whole body exposure to one erythemal dose, it is believed that 250 micrograms/day (10,000 IU) in healthy adults are safe and can thus be adopted as the tolerable upper limit.
Published cases of toxicity involving hypercalcemia in which the vitamin D dose and the 25-hydroxy-vitamin D levels are known all involve an intake of ≥40,000 IU (1000 mcg) per day. Recommending supplementation, when those supposedly in need of it are labeled healthy, has proved contentious, and doubt exists concerning long term effects of attaining and maintaining serum 25(OH)D of at least 80 nmol/L by supplementation. A Toronto study concluded, "skin pigmentation, assessed by measuring skin melanin content, showed an inverse relationship with serum 25(OH)D."
The uniform occurrence of low serum 25(OH)D in Indians living in India and Chinese in China, does not support the hypothesis that the low levels seen in the more pigmented are due to lack of synthesis from the sun at higher latitudes; the leader of the study has urged dark-skinned immigrants to take vitamin D supplements nonetheless, saying, "I see no risk, no downside, there's only a potential benefit."
Dietary reference intakes
Different institutions propose different recommendations concerning daily amounts of the vitamin.Australia and New Zealand
Australia and New Zealand have established average intakes for vitamin D, as follows:Children 5.0 μg /day
Adults 19–50 yr 5.0 μg/day, 51–70 yr 10.0 μg/day, >70 yr 15.0 μg/day
European Union
The recommended daily amount for vitamin D in the European Union is 5 µg.Canada
1 µg = 40 IUInternational unit
In pharmacology, the International Unit is a unit of measurement for the amount of a substance, based on biological activity or effect. It is abbreviated as IU, as UI , or as IE...
and 0.025 µg = 1 IU.
The new reference intakes for vitamin D are:
- 1–70 years of age: 600 IU/day (15 μg/day)
- 71+ years of age: 800 IU/day (20 μg/day)
- Pregnant/lactating: 600 IU/day (15 μg/day)
The reference AI for infants remains at:
- 0–12 months: 400 IU/day (10 μg/day)
Comment
The Dietary Reference IntakeDietary Reference Intake
The Dietary Reference Intake is a system of nutrition recommendations from the Institute of Medicine of the U.S. National Academy of Sciences. The DRI system is used by both the United States and Canada and is intended for the general public and health professionals...
for vitamin D issued by the American (U.S.) Institute of Medicine
Institute of Medicine
The Institute of Medicine is a not-for-profit, non-governmental American organization founded in 1970, under the congressional charter of the National Academy of Sciences...
(IOM) in 2010 superseded a previous recommendation which had Adequate Intake status. The recommendations were formed assuming the individual has no skin synthesis of vitamin D because of inadequate sun exposure. The reference intake for vitamin D refers to total intake from food, beverages and supplements, is intended for the North American population, and assumes that calcium requirements are being met.
One school of thought contends that human physiology is fine tuned to an intake of 4000–12,000 IU/day from sun exposure with concomitant serum 25-hydroxyvitamin D levels of 40 to 80 ng/mL and that this is required for optimal health. Proponents of this view, who include some members of the panel that drafted a now superseded 1997 report on vitamin D from the Institute of Medicine, contend that the IOM's warning about serum concentrations above 50 ng/mL lacks biological plausibility. They suggest that for some people reducing the risk of preventable disease requires a higher level of vitamin D than that recommended by the IOM.
Upper intake levels
The Tolerable Upper Intake Level is defined as "the highest average daily intake of a nutrient that is likely to pose no risk of adverse health effects for nearly all persons in the general population ." Although tolerable upper intake levels are believed to be safe, information on the long term effects is incomplete and these levels of intake are not recommended :- 0–6 months of age: 1,000 IU
- 6–12 months of age: 1,500 IU
- 1–3 years of age: 2,500 IU
- 4–8 years of age: 3,000 IU
- 9-71+ years of age: 4,000 IU
- Pregnant/lactating: 4,000 IU
Serum 25-hydroxyvitamin D
An (U.S.) Institute of Medicine committee concluded that a serum 25-hydroxyvitamin D level of 20 ng/mL is desirable for bone and overall health. The Dietary Reference IntakeDietary Reference Intake
The Dietary Reference Intake is a system of nutrition recommendations from the Institute of Medicine of the U.S. National Academy of Sciences. The DRI system is used by both the United States and Canada and is intended for the general public and health professionals...
s for vitamin D are chosen with a margin of safety and 'overshoot' the targeted serum value to ensure that the specified levels of intake achieve the desired serum 25-hydroxyvitamin D levels in almost all persons. It is assumed there are no contributions to serum 25-hydroxyvitamin D level from sun exposure and the recommendations are fully applicable to people with dark skin or negligible exposure to sunlight.
The Institute found that serum 25-hydroxyvitamin D concentrations above 30 ng/mL are "not consistently associated with increased
benefit". Serum 25-hydroxyvitamin D levels above 50 ng/mL may be cause for concern.
Dietary sources
In some countries, staple foods are artificially fortified with vitamin D. Dietary sources of vitamin D include:- Fatty fish species, such as:
- CatfishCatfishCatfishes are a diverse group of ray-finned fish. Named for their prominent barbels, which resemble a cat's whiskers, catfish range in size and behavior from the heaviest and longest, the Mekong giant catfish from Southeast Asia and the second longest, the wels catfish of Eurasia, to detritivores...
, 85 g (3 oz) provides (5 IU/g) - SalmonSalmonSalmon is the common name for several species of fish in the family Salmonidae. Several other fish in the same family are called trout; the difference is often said to be that salmon migrate and trout are resident, but this distinction does not strictly hold true...
, cooked, 100 g (3.5 oz) provides 360 IU (3.6 IU/g) - MackerelMackerelMackerel is a common name applied to a number of different species of fish, mostly, but not exclusively, from the family Scombridae. They may be found in all tropical and temperate seas. Most live offshore in the oceanic environment but a few, like the Spanish mackerel , enter bays and can be...
, cooked, 100 g (3.5 oz), 345 IU (3.45 IU/g) - SardineSardineSardines, or pilchards, are several types of small, oily fish related to herrings, family Clupeidae. Sardines are named after the Mediterranean island of Sardinia, around which they were once abundant....
s, canned in oil, drained, 50 g (1.75 oz), 250 IU (5 IU/g) - TunaTunaTuna is a salt water fish from the family Scombridae, mostly in the genus Thunnus. Tuna are fast swimmers, and some species are capable of speeds of . Unlike most fish, which have white flesh, the muscle tissue of tuna ranges from pink to dark red. The red coloration derives from myoglobin, an...
, canned in oil, 100 g (3.5 oz), 235 IU (2.35 IU/g) - EelEelEels are an order of fish, which consists of four suborders, 20 families, 111 genera and approximately 800 species. Most eels are predators...
, cooked, 100 g (3.5 oz), 200 IU (2.00 IU/g)
- Catfish
- A whole eggEgg (food)Eggs are laid by females of many different species, including birds, reptiles, amphibians, and fish, and have probably been eaten by mankind for millennia. Bird and reptile eggs consist of a protective eggshell, albumen , and vitellus , contained within various thin membranes...
provides 20 IU if egg weighs 60 g (3 IU/g) - Beef liver, cooked, 100 g (3.5 oz), provides 15 IU (0.15 IU/g)
- Fish liver oils, such as cod liver oilCod liver oilCod liver oil is a nutritional supplement derived from liver of cod fish. It has high levels of the omega-3 fatty acids, EPA and DHA, and very high levels of vitamin A and vitamin D. It is widely taken to ease the symptoms of arthritis and for other health benefits...
, provides (90.6 IU/ml) - UV-irradiated mushrooms and yeastYeastYeasts are eukaryotic micro-organisms classified in the kingdom Fungi, with 1,500 species currently described estimated to be only 1% of all fungal species. Most reproduce asexually by mitosis, and many do so by an asymmetric division process called budding...
are the only known vegan significant sources of vitamin D from food sources. Exposure of portabella mushrooms to UV provides an increase of vitamin D content in an 100-g portion (grilled) from about 14 IU (0.14 IU/g non-exposed) to about 500 IU (5 IU/g exposed to UV light).
Industrial production
Vitamin D3 (cholecalciferol) is produced industrially by exposing 7-dehydrocholesterol7-Dehydrocholesterol
7-Dehydrocholesterol is a zoosterol that functions in the serum as a cholesterol precursor, and is converted to vitamin D3 in the skin, therefore functioning as provitamin-D3. The presence of this compound in human skin enables humans to manufacture vitamin D3 from ultra-violet rays in the sun...
to UVB light, followed by purification. The 7-dehydrocholesterol is a natural substance in wool grease (lanolin
Lanolin
Lanolin , also called Adeps Lanae, wool wax or wool grease, is a yellow waxy substance secreted by the sebaceous glands of wool-bearing animals. Most lanolin used by humans comes from domestic sheep...
) from sheep or other woolly animals. Vitamin D 2 (ergocalciferol) is produced in a similar way using ergosterol from yeast or mushrooms as a starting material.
Synthesis
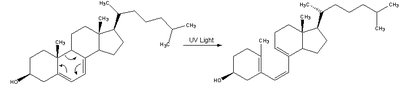
| In the skin, 7-dehydrocholesterol, a derivative of cholesterol Cholesterol Cholesterol is a complex isoprenoid. Specifically, it is a waxy steroid of fat that is produced in the liver or intestines. It is used to produce hormones and cell membranes and is transported in the blood plasma of all mammals. It is an essential structural component of mammalian cell membranes... , is photolyzed Photochemistry Photochemistry, a sub-discipline of chemistry, is the study of chemical reactions that proceed with the absorption of light by atoms or molecules.. Everyday examples include photosynthesis, the degradation of plastics and the formation of vitamin D with sunlight.-Principles:Light is a type of... by ultraviolet light in a 6-electronconrotatory electrocyclic reaction Electrocyclic reaction In organic chemistry, an electrocyclic reaction is a type of pericyclic rearrangement reaction where the net result is one pi bond being converted into one sigma bond or vice-versa... . The product is previtamin D3 Previtamin D3 Previtamin D3 is an intermediate in the production of vitamin D.... . |
 |
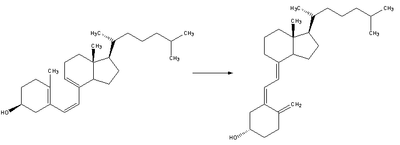
| Previtamin D3 spontaneously isomer Isomer In chemistry, isomers are compounds with the same molecular formula but different structural formulas. Isomers do not necessarily share similar properties, unless they also have the same functional groups. There are many different classes of isomers, like stereoisomers, enantiomers, geometrical... izes to vitamin D 3 (cholecalciferol Cholecalciferol Cholecalciferol is a form of vitamin D, also called vitamin D3 or calciol.It is structurally similar to steroids such as testosterone, cholesterol, and cortisol .-Forms:Vitamin D3 has several forms:... ) in a antarafacial sigmatropic [1,7] hydride shift. At room temperature, the transformation of previtamin D3 to vitamin D3 takes about 12 days to complete. |
 |
| Whether it is made in the skin or ingested, cholecalciferol is hydroxylated in the liver Liver The liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion... at position 25 (upper right of the molecule) to form 25-hydroxycholecalciferol (calcidiol or 25(OH)D). This reaction is catalyzed by the microsomal Microsome In cell biology, microsomes are vesicle-like artifacts re-formed from pieces of the endoplasmic reticulum when eukaryotic cells are broken-up in the laboratory; by definition, microsomes are not ordinarily present in living cells.... enzyme vitamin D 25-hydroxylase, which is produced by hepatocytes. Once made, the product is released into the plasma, where it is bound to an α-globulin, vitamin D binding protein. |
|
| Calcidiol is transported to the proximal tubules of the kidneys, where it is hydroxylated at the 1-α position (lower right of the molecule) to formcalcitriol Calcitriol Calcitriol , also called 1,25-dihydroxycholecalciferol or 1,25-dihydroxyvitamin D3, is the hormonally active form of vitamin D with three hydroxyl groups... (aka 1,25-dihydroxycholecalciferol and abbreviated to 1,25(OH)2D). This product is a potent ligand Ligand In coordination chemistry, a ligand is an ion or molecule that binds to a central metal atom to form a coordination complex. The bonding between metal and ligand generally involves formal donation of one or more of the ligand's electron pairs. The nature of metal-ligand bonding can range from... of the vitamin D receptor (VDR), which mediates most of the physiological actions of the vitamin. The conversion of calcidiol to calcitriol is catalyzed by the enzyme25-hydroxyvitamin D3 1-alpha-hydroxylase 25-Hydroxyvitamin D3 1-alpha-hydroxylase 25-Hydroxyvitamin D3 1-alpha-hydroxylase also known as cytochrome p450 27B1 is a cytochrome P450 enzyme that in humans is encoded by the CYP27B1 gene.... , the levels of which are increased by parathyroid hormone Parathyroid hormone Parathyroid hormone , parathormone or parathyrin, is secreted by the chief cells of the parathyroid glands as a polypeptide containing 84 amino acids... (and additionally by low calcium or phosphate). |
Tuberculosis
Historically, vitamin D3 was used to treat tuberculosis patients, but has not been adequately investigated in controlled clinical trials. The hormonally active form of vitamin D3, 1,25-dihydroxycholecalciferol (1,25(OH)2D), has been shown to have antimycobacterialAntimycobacterial
An antimycobacterial is a type of drug used to treat Mycobacteria infections.Types include:* Tuberculosis treatments* Leprostatic agents...
activity in vitro
In vitro
In vitro refers to studies in experimental biology that are conducted using components of an organism that have been isolated from their usual biological context in order to permit a more detailed or more convenient analysis than can be done with whole organisms. Colloquially, these experiments...
, but the applicability of this effect to clinical situations has not been shown.
Vitamin D3 supplementations have not shown any improvement in treating tuberculosis except in a small subset of patients with the tt genotype of the TaqI vitamin D receptor polymorphism. Several studies have shown an association between low serum levels of 25-hydroxycholecalciferol (25(OH)D) and increased risk for both active tuberculosis
Tuberculosis
Tuberculosis, MTB, or TB is a common, and in many cases lethal, infectious disease caused by various strains of mycobacteria, usually Mycobacterium tuberculosis. Tuberculosis usually attacks the lungs but can also affect other parts of the body...
disease progression and susceptibility. More prospective studies will be required to ascertain the potential role of vitamin D supplementation in treating patients with tuberculosis.
HIV
Vitamin D3 has also shown some anti-HIVHIV
Human immunodeficiency virus is a lentivirus that causes acquired immunodeficiency syndrome , a condition in humans in which progressive failure of the immune system allows life-threatening opportunistic infections and cancers to thrive...
-1 effects in vitro, including the induction of autophagy
Autophagy
In cell biology, autophagy, or autophagocytosis, is a catabolic process involving the degradation of a cell's own components through the lysosomal machinery. It is a tightly regulated process that plays a normal part in cell growth, development, and homeostasis, helping to maintain a balance...
. The potential effect in humans has not been investigated. Lower levels of 1,25(OH)2D in HIV infected patients are correlated with significantly lower CD4+ T cell counts and higher tumor necrosis factor
Tumor necrosis factor
Tumor necrosis factor is a cytokine involved in systemic inflammation and is a member of a group of cytokines that stimulate the acute phase reaction...
levels, which normally decrease in number with progression to AIDS
AIDS
Acquired immune deficiency syndrome or acquired immunodeficiency syndrome is a disease of the human immune system caused by the human immunodeficiency virus...
, although no causative association has been shown. In an epidemiological study of HIV positive women in Tanzania, there appeared to be a correlation between reduced levels of vitamin D and speed of HIV disease progression. These results will need to be confirmed in a blinded clinical trial before dietary recommendations can be made.
Further reading
Books- Holick, M.F. (2011). The Vitamin D Solution. Plume (Penguin Group). ISBN 9780452296886
- Ross, A.C/Taylor, C.L./Yaktine, A.L./Valle, H.B.D. (editors, 2011) Dietary Reference Intakes for Calcium and Vitamin D. National Academies Press. ISBN 9780309163941
- Rubin, A.L. (2011). Vitamin D for Dummies. Wiley Publishing. ISBN 9780470891759
Review articles
- Davis, C.D. / Milner, J.A. "Nutrigenomics, Vitamin D and Cancer Prevention",Journal of Nutrigenetics and Nutrigenomics (2011),4(1):1-11. Nutritional Science Research Group, National Cancer Institute (NCI)
- Thacher, T.D. / Clarke, B.L. "Vitamin D insufficiency", Majo Clinic Proceedings (2011),86(1):50-60.
- Zhang, R. / Naughton, D.P. "Vitamin D in health and disease: Current perspectives", Nutrition Journal (2010),9:65.
External links
- Dietary Supplement Fact Sheet: Vitamin D from the U.S. National Institutes of HealthNational Institutes of HealthThe National Institutes of Health are an agency of the United States Department of Health and Human Services and are the primary agency of the United States government responsible for biomedical and health-related research. Its science and engineering counterpart is the National Science Foundation...
- Disagreement among experts about the correct vitamin D dose. (Nature News, July 6, 2011)