

Oxygen toxicity
Encyclopedia
Oxygen toxicity is a condition resulting from the harmful effects of breathing molecular oxygen
at elevated partial pressure
s. It is also known as oxygen toxicity syndrome, oxygen intoxication, and oxygen poisoning. Historically, the central nervous system
condition was called the Paul Bert
effect, and the pulmonary condition the Lorrain Smith effect, after the researchers who pioneered its discovery and description in the late 19th century. Severe cases can result in cell
damage and death, with effects most often seen in the central nervous system, lung
s and eyes. Oxygen toxicity is a concern for scuba divers, those on high concentrations of supplemental oxygen (particularly premature babies), and those undergoing hyperbaric oxygen therapy
.
The result of breathing elevated concentrations of oxygen is hyperoxia, an excess of oxygen in body tissues. The body is affected in different ways depending on the type of exposure. Central nervous system toxicity is caused by short exposure to high concentrations of oxygen at greater than atmospheric pressure. Pulmonary and ocular toxicity result from longer exposure to elevated oxygen levels at normal pressure. Symptoms may include disorientation, breathing problems, and vision changes such as myopia
. Prolonged or very high oxygen concentrations can cause oxidative damage to cell membranes, the collapse of the alveoli in the lungs, retinal detachment
, and seizures. Oxygen toxicity is managed by reducing the exposure to elevated oxygen levels. Studies show that, in the long term, a robust recovery from most types of oxygen toxicity is possible.
Protocols for avoidance of hyperoxia exist in fields where oxygen is breathed at higher-than-normal partial pressures, including underwater diving
using compressed breathing gases, hyperbaric medicine, neonatal care and human spaceflight
. These protocols have resulted in the increasing rarity of seizures due to oxygen toxicity, with pulmonary and ocular damage being mainly confined to the problems of managing premature infants.
In recent years, oxygen has become available for recreational use in oxygen bar
s. The US Food and Drug Administration has warned those suffering from problems such as heart or lung disease not to use oxygen bars. Scuba divers use breathing gases containing up to 100% oxygen, and should have specific training in using such gases.
Central nervous system oxygen toxicity can cause seizures, brief periods of rigidity followed by convulsions and unconsciousness, and is of concern to divers who encounter greater than atmospheric pressures. Pulmonary oxygen toxicity results in damage to the lungs, causing pain and difficulty in breathing. Oxidative damage to the eye may lead to myopia or partial detachment of the retina
. Pulmonary and ocular damage are most likely to occur when supplemental oxygen is administered as part of a treatment, particularly to newborn infants, but are also a concern during hyperbaric oxygen therapy.
Oxidative damage may occur in any cell in the body but the effects on the three most susceptible organs will be the primary concern. It may also be implicated in red blood cell destruction (haemolysis
), damage to liver (hepatic), heart (myocardial), endocrine
glands (adrenal
, gonad
s, and thyroid
), or kidneys (renal), and general damage to cells
.
In unusual circumstances, effects on other tissues may be observed: it is suspected that during spaceflight, high oxygen concentrations may contribute to bone damage. Hyperoxia can also indirectly cause carbon dioxide narcosis
in patients with lung ailments such as chronic obstructive pulmonary disease
or with central respiratory depression. Oxygen toxicity is not associated with hyperventilation
, because breathing air at atmospheric pressure always has a partial pressure of oxygen (ppO2) of 0.21 bar (21,000 Pa) and the lower limit for toxicity is more than 0.3 bar (30,000 Pa).
oxygen toxicity manifests as symptoms such as visual changes (especially tunnel vision
), ringing in the ears (tinnitus
), nausea
, twitching (especially of the face), irritability (personality changes, anxiety
, confusion, etc.), and dizziness
. This may be followed by a tonic–clonic seizure consisting of two phases: intense muscle contraction occurs for several seconds (tonic); followed by rapid spasms of alternate muscle relaxation and contraction producing convulsive jerking (clonic). The seizure ends with a period of unconsciousness (the postictal state
). The onset of seizure depends upon the partial pressure of oxygen (ppO2) in the breathing gas
and exposure duration. However, exposure time before onset is unpredictable, as tests have shown a wide variation, both amongst individuals, and in the same individual from day to day.
In addition, many external factors, such as underwater immersion, exposure to cold, and exercise will decrease the time to onset of central nervous system symptoms.
Decrease of tolerance is closely linked to retention of carbon dioxide
. Other factors, such as darkness and caffeine
, increase tolerance in test animals, but these effects have not been proven in humans.
). The symptoms appear in the upper chest region (substernal and carinal
regions).
This begins as a mild tickle on inhalation and progresses to frequent coughing. If breathing elevated partial pressures of oxygen is not discontinued, patients experience a mild burning on inhalation along with uncontrollable coughing and occasional shortness of breath (dyspnoea
). Physical findings related to pulmonary toxicity have included bubbling sounds heard through a stethoscope
(bubbling rales
), fever, and increased blood flow to the lining of the nose (hyperaemia
of the nasal mucosa). The radiological finding from the lungs shows inflammation
and swelling (pulmonary oedema
). Pulmonary function measurements
are reduced, as noted by a reduction in the amount of air that the lungs can hold (vital capacity
) and changes in expiratory function and lung elasticity. Tests in animals have indicated a variation in tolerance similar to that found in central nervous system toxicity, as well as significant variations between species. When the exposure to oxygen above 0.5 bar (50,000 Pa) is intermittent, it permits the lungs to recover and delays the onset of toxicity.
, or ROP) are observed via an ophthalmoscope as a demarcation between the vascularised and non-vascularised regions of an infant's retina. The degree of this demarcation is used to designate four stages: (I) the demarcation is a line; (II) the demarcation becomes a ridge; (III) growth of new blood vessels occurs around the ridge; (IV) the retina begins to detach from the inner wall of the eye (choroid
).
are markedly different.
is above normal. Divers breathing air at depths greater than 60 m (196.9 ft) face an increasing risk of an oxygen toxicity "hit" (seizure). Divers breathing a gas mixture enriched with oxygen, such as nitrox, can similarly suffer a seizure at shallower depths, should they descend below the maximum depth allowed for the mixture.
, are exposed to the highest concentration of oxygen in the human body and are therefore the first organs to show toxicity. Pulmonary toxicity occurs with exposure to concentrations of oxygen greater than 0.5 bar (50,000 Pa), corresponding to an oxygen fraction of 50% at normal atmospheric pressure. Signs of pulmonary toxicity begins with evidence of tracheobronchitis, or inflammation of the upper airways, after an asymptomatic period between 4 and 22 hours at greater than 95% oxygen, with some studies suggesting symptoms usually begin after approximately 14 hours at this level of oxygen.
At partial pressures of oxygen of 2 bar—100% oxygen at 2 to 3 times atmospheric pressure—these symptoms may begin as early as 3 hours after exposure to oxygen. Experiments on rats show pulmonary manifestations of oxygen toxicity are not the same for normobaric conditions as they are for hyperbaric conditions. Evidence of decline in lung function as measured by pulmonary function testing can occur as quickly as 24 hours of continuous exposure to 100% oxygen, with evidence of diffuse alveolar damage
and the onset of acute respiratory distress syndrome
usually occurring after 48 hours on 100% oxygen. Breathing 100% oxygen also eventually leads to collapse of the alveoli (atelectasis
), while—at the same partial pressure of oxygen—the presence of significant partial pressures of inert gases, typically nitrogen, will prevent this effect.
Preterm newborns are known to be at higher risk for bronchopulmonary dysplasia
with extended exposure to high concentrations of oxygen. Other groups at higher risk for oxygen toxicity are patients on mechanical ventilation
with exposure to levels of oxygen greater than 50%, and patients exposed to chemicals that increase risk for oxygen toxicity such the chemotherapeutic agent bleomycin
. Therefore, current guidelines for patients on mechanical ventilation in intensive care suggests keeping oxygen concentration less than 60%. Likewise, divers who undergo treatment of decompression sickness
are at increased risk of oxygen toxicity as treatment entails exposure to long periods of oxygen breathing under hyperbaric conditions, in addition to any oxygen exposure during the dive.
.
Damage to the developing eye of infants exposed to high oxygen fraction at normal pressure has a different mechanism and effect from the eye damage experienced by adult divers under hyperbaric conditions.
Hyperoxia may be a contributing factor for the disorder called retrolental fibroplasia or retinopathy of prematurity (ROP) in infants.
In preterm infants, the retina is often not fully vascularised. Retinopathy of prematurity occurs when the development of the retinal vasculature is arrested and then proceeds abnormally. Associated with the growth of these new vessels is fibrous tissue
(scar tissue) that may contract to cause retinal detachment. Supplemental oxygen exposure, while a risk factor
, is not the main risk factor for development of this disease. Restricting supplemental oxygen use does not necessarily reduce the rate of retinopathy of prematurity, and may raise the risk of hypoxia-related systemic complications.
Hyperoxic myopia
has occurred in closed circuit oxygen rebreather divers with prolonged exposures.
It also occurs frequently in those undergoing repeated hyperbaric oxygen therapy. This is due to an increase in the refractive power of the lens
, since axial length and keratometry
readings do not reveal a cornea
l or length basis for a myopic shift. It is usually reversible with time.
 The biochemical basis for the toxicity of oxygen is the partial reduction of oxygen by one or two electrons to form reactive oxygen species, which are natural by-products of the normal metabolism
The biochemical basis for the toxicity of oxygen is the partial reduction of oxygen by one or two electrons to form reactive oxygen species, which are natural by-products of the normal metabolism
of oxygen and have important roles in cell signalling.
One species produced by the body, the superoxide
anion (O2–), is possibly involved in iron acquisition.
Higher than normal concentrations of oxygen lead to increased levels of reactive oxygen species.
Oxygen is necessary for cell metabolism, and the blood supplies it to all parts of the body. When oxygen is breathed at high partial pressures, a hyperoxic condition will rapidly spread, with the most vascularised tissues being most vulnerable.
During times of environmental stress, levels of reactive oxygen species can increase dramatically, which can damage cell structures and produce oxidative stress
.
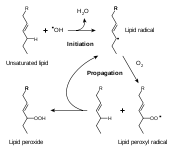
While all the reaction mechanisms of these species within the body are not yet fully understood,
one of the most reactive products of oxidative stress is the hydroxyl radical
(·OH), which can initiate a damaging chain reaction of lipid peroxidation
in the unsaturated lipids within cell membranes.
High concentrations of oxygen also increase the formation of other free radicals, such as nitric oxide
, peroxynitrite
, and trioxidane
, which harm DNA
and other biomolecules.
Although the body has many antioxidant
systems such as glutathione
that guard against oxidative stress, these systems are eventually overwhelmed at very high concentrations of free oxygen, and the rate of cell damage exceeds the capacity of the systems that prevent or repair it. Cell damage and cell death then result.
, congestion and coldness. However, these symptoms may be helpful in diagnosing the first stages of oxygen toxicity in patients undergoing hyperbaric oxygen therapy. In either case, unless there is a prior history of epilepsy
or tests indicate hypoglycaemia
, a seizure occurring in the setting of breathing oxygen at partial pressures greater than 1.4 bar (140,000 Pa) suggests a diagnosis of oxygen toxicity.
Diagnosis of bronchopulmonary dysplasia in new-born infants with breathing difficulties is difficult in the first few weeks. However, if the infant's breathing does not improve during this time, blood tests and x-rays may be used to confirm bronchopulmonary dysplasia. In addition, an echocardiogram can help to eliminate other possible causes such as congenital heart defects or pulmonary arterial hypertension.
The diagnosis of retinopathy of prematurity in infants is typically suggested by the clinical setting. Prematurity, low birth weight and a history of oxygen exposure are the principal indicators, while no hereditary factors have been shown to yield a pattern.
 The prevention of oxygen toxicity depends entirely on the setting. Both underwater and in space, proper precautions can eliminate the most pernicious effects. Premature infants commonly require supplemental oxygen to treat complications of preterm birth. In this case prevention of bronchopulmonary dysplasia and retinopathy of prematurity must be carried out without compromising a supply of oxygen adequate to preserve the infant's life.
The prevention of oxygen toxicity depends entirely on the setting. Both underwater and in space, proper precautions can eliminate the most pernicious effects. Premature infants commonly require supplemental oxygen to treat complications of preterm birth. In this case prevention of bronchopulmonary dysplasia and retinopathy of prematurity must be carried out without compromising a supply of oxygen adequate to preserve the infant's life.
. The diver may experience no warning symptoms. The effects are sudden convulsions and unconsciousness, during which victims can lose their regulator
and drown. One of the advantages of a full-face diving mask is prevention of regulator loss in the event of a seizure. As there is an increased risk of central nervous system oxygen toxicity on deep dives, long dives and dives where oxygen-rich breathing gases are used, divers are taught to calculate a maximum operating depth
for oxygen-rich breathing gas
es, and cylinders containing such mixtures must be clearly marked with that depth.
In some diver training
courses for these types of diving, divers are taught to plan and monitor what is called the oxygen clock of their dives. This is a notional alarm clock, which ticks more quickly at increased ppO2 and is set to activate at the maximum single exposure limit recommended in the National Oceanic and Atmospheric Administration
Diving Manual. For the following partial pressures of oxygen the limit is: 45 minutes at 1.6 bar (160,000 Pa), 120 minutes at 1.5 bar (150,000 Pa), 150 minutes at 1.4 bar (140,000 Pa), 180 minutes at 1.3 bar (130,000 Pa) and 210 minutes at 1.2 bar (120,000 Pa), but is impossible to predict with any reliability whether or when toxicity symptoms will occur.
Many nitrox-capable dive computer
s calculate an oxygen loading and can track it across multiple dives. The aim is to avoid activating the alarm by reducing the ppO2 of the breathing gas or the length of time breathing gas of higher ppO2. As the ppO2 depends on the fraction of oxygen in the breathing gas and the depth of the dive, the diver obtains more time on the oxygen clock by diving at a shallower depth, by breathing a less oxygen-rich gas, or by shortening the duration of exposure to oxygen-rich gases.
Diving below 60 m (196.9 ft) on air would expose a diver to increasing danger of oxygen toxicity as the partial pressure of oxygen exceeds 1.4 bar (140,000 Pa), so a gas mixture must be used which contains less than 21% oxygen (a hypoxic mixture). Increasing the proportion of nitrogen
is not viable, since it would produce a strongly narcotic
mixture. However, helium
is not narcotic, and a usable mixture may be blended
either by completely replacing nitrogen with helium (the resulting mix is called heliox
), or by replacing part of the nitrogen with helium, producing a trimix.
Pulmonary oxygen toxicity is an entirely avoidable event while diving. The limited duration and naturally intermittent nature of most diving makes this a relatively rare (and even then, reversible) complication for divers. Guidelines have been established that allow divers to calculate when they are at risk of pulmonary toxicity.
allow for periods of breathing air rather than 100% oxygen (oxygen breaks) to reduce the chance of seizure or lung damage. The U.S. Navy uses treatment tables based on periods alternating between 100% oxygen and air. For example, U.S.N. table 6 requires 75 minutes (three periods of 20 minutes oxygen/5 minutes air) at an ambient pressure of 2.8 standard atmospheres (283,710 Pa), equivalent to a depth of 18 metres (59.1 ft). This is followed by a slow reduction in pressure to 1.9 atm (192,517.5 Pa) over 30 minutes on oxygen. The patient then remains at that pressure for a further 150 minutes, consisting of two periods of 15 minutes air/60 minutes oxygen, before the pressure is reduced to atmospheric over 30 minutes on oxygen.
Vitamin E
and selenium
were proposed and later rejected as a potential method of protection against pulmonary oxygen toxicity.
There is however some experimental evidence in rats that vitamin E and selenium aid in preventing in vivo
lipid peroxidation
and free radical damage, and therefore prevent retinal changes following repetitive hyperbaric oxygen exposures.
Retinopathy of prematurity is largely preventable by screening. Current guidelines require that all babies of less than 32 weeks gestational age
or having a birth weight less than 1.5 kg (3.3 lb) should be screened for retinopathy of prematurity at least every two weeks.
The National Cooperative Study in 1954 showed a causal link between supplemental oxygen and retinopathy of prematurity, but subsequent curtailment of supplemental oxygen caused an increase in infant mortality. To balance the risks of hypoxia
and retinopathy of prematurity, modern protocols now require monitoring of blood oxygen levels in premature infants receiving oxygen.
and Apollo spacecraft
).
In such applications as extra-vehicular activity
, high-fraction oxygen is non-toxic, even at breathing mixture fractions approaching 100%, because the oxygen partial pressure is not allowed to chronically
exceed 0.3 bar (4.4 psi).

 During hyperbaric oxygen therapy, the patient will usually breathe 100% oxygen from a mask, while inside a hyperbaric chamber pressurised with air to about 2.8 bar (280,000 Pa). Seizures during the therapy are managed by removing the mask from the patient, thereby dropping the partial pressure of oxygen inspired below 0.6 bar (60,000 Pa).
During hyperbaric oxygen therapy, the patient will usually breathe 100% oxygen from a mask, while inside a hyperbaric chamber pressurised with air to about 2.8 bar (280,000 Pa). Seizures during the therapy are managed by removing the mask from the patient, thereby dropping the partial pressure of oxygen inspired below 0.6 bar (60,000 Pa).
A seizure underwater requires that the diver is brought to the surface as soon as practicable. Although for many years the recommendation has been not to raise the diver during the seizure itself, owing to the danger of arterial gas embolism, there is no evidence of expiratory obstruction during seizure and benefit may be gained by raising the diver during the seizure's clonic phase.
Rescuers need to ensure that their own safety is not compromised during the convulsive phase. They then ensure that the victim's air supply is established and maintained, and carry out a controlled buoyant lift
. Lifting an unconscious body is taught by most diver training
agencies. Upon reaching the surface, emergency services are always contacted as there is a possibility of further complications requiring medical attention. The U.S. Navy has procedures for completing the decompression stops where a recompression chamber is not immediately available.
The occurrence of symptoms of bronchopulmonary dysplasia or acute respiratory distress syndrome is treated by lowering the fraction of oxygen administered, along with a reduction in the periods of exposure and an increase in the break periods where normal air is supplied. Where supplemental oxygen is required for treatment of another disease (particularly in infants), a ventilator may be needed to ensure that the lung tissue remains inflated. Reductions in pressure and exposure will be made progressively and medications such as bronchodilators and pulmonary surfactant
s may be used.
Retinopathy of prematurity may regress
spontaneously, but should the disease progress beyond a threshold (defined as five contiguous or eight cumulative hours of stage 3 retinopathy of prematurity), both cryosurgery
and laser surgery
have been shown to reduce the risk of blindness as an outcome. Where the disease has progressed further, techniques such as scleral buckling
and vitrectomy
surgery may assist in re-attaching the retina.
The majority of infants who have survived following an incidence of bronchopulmonary dysplasia will eventually recover near-normal lung function, since lungs continue to grow during the first 5–7 years and the damage caused by bronchopulmonary dysplasia is to some extent reversible (even in adults). However, they are likely be more susceptible to respiratory infections for the rest of their lives and the severity of later infections is often greater than that in their peers.
Retinopathy of prematurity (ROP) in infants frequently regresses without intervention and eyesight may be normal in later years. Where the disease has progressed to the stages requiring surgery, the outcomes are generally good for the treatment of stage 3 ROP, but are much worse for the later stages. Although surgery is usually successful in restoring the anatomy of the eye, damage to the nervous system by the progression of the disease leads to comparatively poorer results in restoring vision. The presence of other complicating diseases also reduces the likelihood of a favourable outcome.
The variability in tolerance and other variable factors such as workload have resulted in the U.S. Navy abandoning screening for oxygen tolerance. Of the 6,250 oxygen-tolerance tests performed between 1976 and 1997, only 6 episodes of oxygen toxicity were observed (0.1%).
Central nervous system oxygen toxicity among patients undergoing hyperbaric oxygen therapy is rare, and is influenced by a number of a factors: individual sensitivity and treatment protocol; and probably therapy indication
and equipment used. A study by Welslau in 1996 reported 16 incidents out of a population of 107,264 patients (0.015%), while Hampson and Atik in 2003 found a rate of 0.03%. Yildiz, Ay and Qyrdedi, in a summary of 36,500 patient treatments between 1996 and 2003, reported only 3 oxygen toxicity incidents, giving a rate of 0.008%. A later review of over 80,000 patient treatments revealed an even lower rate: 0.0024%. The reduction in incidence may be partly due to use of a mask (rather than a hood) to deliver oxygen.
Bronchopulmonary dysplasia is among the most common complications of prematurely born
infants and its incidence has grown as the survival of extremely premature infants has increased. Nevertheless, the severity has decreased as better management of supplemental oxygen has resulted in the disease now being related mainly to factors other than hyperoxia.
In 1997 a summary of studies of neonatal intensive care units in industrialised countries showed that up to 60% of low birth weight
babies developed retinopathy of prematurity, which rose to 72% in extremely low birth weight babies, defined as less than 1 kg (2.2 lb) at birth. However, severe outcomes are much less frequent: for very low birth weight babies—those less than 1.5 kg (3.3 lb) at birth—the incidence of blindness was found to be no more than 8%.
 Central nervous system toxicity was first described by Paul Bert
Central nervous system toxicity was first described by Paul Bert
in 1878.
He showed that oxygen was toxic to insects, arachnids, myriapods
, molluscs, earthworms, fungi, germinating seeds, birds, and other animals. Central nervous system toxicity may be referred to as the "Paul Bert effect".
Pulmonary oxygen toxicity was first described by J. Lorrain Smith in 1899 when he noted central nervous system toxicity and discovered in experiments in mice and birds that 0.43 bar (43,000 Pa) had no effect but 0.75 bar (75,000 Pa) of oxygen was a pulmonary irritant.
Pulmonary toxicity may be referred to as the "Lorrain Smith effect".
The first recorded human exposure was undertaken in 1910 by Bornstein when two men breathed oxygen at 2.8 bar (280,000 Pa) for 30 minutes while he went on to 48 minutes with no symptoms. In 1912, Bornstein developed cramps in his hands and legs while breathing oxygen at 2.8 bar (280,000 Pa) for 51 minutes.
Smith then went on to show that intermittent exposure to a breathing gas with less oxygen permitted the lungs to recover and delayed the onset of pulmonary toxicity.
Albert R. Behnke
et al. in 1935 were the first to observe visual field
contraction (tunnel vision
) on dives between 1 bar (100,000 Pa) and 4.1 bar (410,000 Pa).
During World War II, Donald and Yarbrough et al. performed over 2,000 experiments on oxygen toxicity to support the initial use of closed circuit oxygen rebreather
s.
Naval divers in the early years of oxygen rebreather diving developed a mythology about a monster called "Oxygen Pete", who lurked in the bottom of the Admiralty Experimental Diving Unit "wet pot" (a water-filled hyperbaric chamber) to catch unwary divers. They called having an oxygen toxicity attack "getting a Pete".
In the decade following World War II, Lambertsen
et al. made further discoveries on the effects of breathing oxygen under pressure as well as methods of prevention.
Their work on intermittent exposures for extension of oxygen tolerance and on a model for prediction of pulmonary oxygen toxicity based on pulmonary function are key documents in the development of standard operating procedures when breathing elevated pressures of oxygen.
Lambertsen's work showing the effect of carbon dioxide in decreasing time to onset of central nervous system symptoms has influenced work from current exposure guidelines to future breathing apparatus
design.
Retinopathy of prematurity was not observed prior to World War II, but with the availability of supplemental oxygen in the decade following, it rapidly became one of the principal causes of infant blindness in developed countries. By 1960 the use of oxygen had become identified as a risk factor and its administration restricted. The resulting fall in retinopathy of prematurity was accompanied by a rise in infant mortality and hypoxia
-related complications. Since then, more sophisticated monitoring and diagnosis have established protocols for oxygen use which aim to balance between hypoxic conditions and problems of retinopathy of prematurity.
Bronchopulmonary dysplasia was first described by Northway in 1967, who outlined the conditions that would lead to the diagnosis.
This was later expanded by Bancalari and in 1988 by Shennan, who suggested the need for supplemental oxygen at 36 weeks could predict long-term outcomes.
Nevertheless, Palta et al. in 1998 concluded that radiographic evidence was the most accurate predictor of long-term effects.
Bitterman et al. in 1986 and 1995 showed that darkness
and caffeine
would delay the onset of changes to brain electrical activity
in rats.
In the years since, research on central nervous system toxicity has centred on methods of prevention and safe extension of tolerance.
Sensitivity to central nervous system oxygen toxicity has been shown to be affected by factors such as circadian rhythm
, drugs, age, and gender.
In 1988, Hamilton et al. wrote procedures for the National Oceanic and Atmospheric Administration to establish oxygen exposure limits for habitat
operations.
Even today, models for the prediction of pulmonary oxygen toxicity do not explain all the results of exposure to high partial pressures of oxygen.
commonly breathe nitrox containing up to 40% oxygen, while technical divers
use pure oxygen or nitrox containing up to 80% oxygen. Divers who breathe oxygen fractions greater than in air (21%) need to be trained in the dangers of oxygen toxicity and how to prevent them. In order to buy nitrox, a diver has to show evidence of such qualification.
Since the late 1990s the recreational use of oxygen has been promoted by oxygen bars, where customers breathe oxygen through a nasal cannula
. Claims have been made that this reduces stress, increases energy, and lessens the effects of hangovers and headaches, despite the lack of any scientific evidence to support them.
There are also devices on sale that offer "oxygen massage" and "oxygen detoxification" with claims of removing body toxins and reducing body fat.
The American Lung Association
has stated "there is no evidence that oxygen at the low flow levels used in bars can be dangerous to a normal person's health", but the U.S. Center for Drug Evaluation and Research
cautions that people with heart or lung disease need their supplementary oxygen carefully regulated and should not use oxygen bars.
Victorian society had a fascination for the rapidly expanding field of science. In "Dr. Ox's Experiment
", a short story written by Jules Verne
in 1872, the eponymous doctor uses electrolysis of water
to separate oxygen and hydrogen. He then pumps the pure oxygen throughout the town of Quiquendone, causing the normally tranquil inhabitants and their animals to become aggressive and plants to grow rapidly. An explosion of the hydrogen and oxygen in Dr Ox's factory brings his experiment to an end. Verne summarised his story by explaining that the effects of oxygen described in the tale were his own invention. There is also a brief episode of oxygen intoxication in his "From the Earth to the Moon
".
The following external site is a compendium of resources:
Specialised
The following external sites contain resources specific to particular topics:
Oxygen
Oxygen is the element with atomic number 8 and represented by the symbol O. Its name derives from the Greek roots ὀξύς and -γενής , because at the time of naming, it was mistakenly thought that all acids required oxygen in their composition...
at elevated partial pressure
Partial pressure
In a mixture of ideal gases, each gas has a partial pressure which is the pressure which the gas would have if it alone occupied the volume. The total pressure of a gas mixture is the sum of the partial pressures of each individual gas in the mixture....
s. It is also known as oxygen toxicity syndrome, oxygen intoxication, and oxygen poisoning. Historically, the central nervous system
Central nervous system
The central nervous system is the part of the nervous system that integrates the information that it receives from, and coordinates the activity of, all parts of the bodies of bilaterian animals—that is, all multicellular animals except sponges and radially symmetric animals such as jellyfish...
condition was called the Paul Bert
Paul Bert
Paul Bert was a French zoologist, physiologist and politician. He is sometimes given the sobriquet "Father of Aviation Medicine".-Life:Bert was born at Auxerre...
effect, and the pulmonary condition the Lorrain Smith effect, after the researchers who pioneered its discovery and description in the late 19th century. Severe cases can result in cell
Cell (biology)
The cell is the basic structural and functional unit of all known living organisms. It is the smallest unit of life that is classified as a living thing, and is often called the building block of life. The Alberts text discusses how the "cellular building blocks" move to shape developing embryos....
damage and death, with effects most often seen in the central nervous system, lung
Lung
The lung is the essential respiration organ in many air-breathing animals, including most tetrapods, a few fish and a few snails. In mammals and the more complex life forms, the two lungs are located near the backbone on either side of the heart...
s and eyes. Oxygen toxicity is a concern for scuba divers, those on high concentrations of supplemental oxygen (particularly premature babies), and those undergoing hyperbaric oxygen therapy
Hyperbaric oxygen therapy
Hyperbaric medicine, also known as hyperbaric oxygen therapy , is the medical use of oxygen at a level higher than atmospheric pressure. The equipment required consists of a pressure chamber, which may be of rigid or flexible construction, and a means of delivering 100% oxygen...
.
The result of breathing elevated concentrations of oxygen is hyperoxia, an excess of oxygen in body tissues. The body is affected in different ways depending on the type of exposure. Central nervous system toxicity is caused by short exposure to high concentrations of oxygen at greater than atmospheric pressure. Pulmonary and ocular toxicity result from longer exposure to elevated oxygen levels at normal pressure. Symptoms may include disorientation, breathing problems, and vision changes such as myopia
Myopia
Myopia , "shortsightedness" ) is a refractive defect of the eye in which collimated light produces image focus in front of the retina under conditions of accommodation. In simpler terms, myopia is a condition of the eye where the light that comes in does not directly focus on the retina but in...
. Prolonged or very high oxygen concentrations can cause oxidative damage to cell membranes, the collapse of the alveoli in the lungs, retinal detachment
Retinal detachment
Retinal detachment is a disorder of the eye in which the retina peels away from its underlying layer of support tissue. Initial detachment may be localized, but without rapid treatment the entire retina may detach, leading to vision loss and blindness. It is a medical emergency.The retina is a...
, and seizures. Oxygen toxicity is managed by reducing the exposure to elevated oxygen levels. Studies show that, in the long term, a robust recovery from most types of oxygen toxicity is possible.
Protocols for avoidance of hyperoxia exist in fields where oxygen is breathed at higher-than-normal partial pressures, including underwater diving
Underwater diving
Underwater diving is the practice of going underwater, either with breathing apparatus or by breath-holding .Recreational diving is a popular activity...
using compressed breathing gases, hyperbaric medicine, neonatal care and human spaceflight
Human spaceflight
Human spaceflight is spaceflight with humans on the spacecraft. When a spacecraft is manned, it can be piloted directly, as opposed to machine or robotic space probes and remotely-controlled satellites....
. These protocols have resulted in the increasing rarity of seizures due to oxygen toxicity, with pulmonary and ocular damage being mainly confined to the problems of managing premature infants.
In recent years, oxygen has become available for recreational use in oxygen bar
Oxygen bar
An oxygen bar is an establishment, or part of one, that sells oxygen for recreational use. Individual flavored scents may be added to enhance the experience...
s. The US Food and Drug Administration has warned those suffering from problems such as heart or lung disease not to use oxygen bars. Scuba divers use breathing gases containing up to 100% oxygen, and should have specific training in using such gases.
Classification
The effects of oxygen toxicity may be classified by the organs affected, producing three principal forms:- Central nervous system, characterised by convulsionsSeizureAn epileptic seizure, occasionally referred to as a fit, is defined as a transient symptom of "abnormal excessive or synchronous neuronal activity in the brain". The outward effect can be as dramatic as a wild thrashing movement or as mild as a brief loss of awareness...
followed by unconsciousness, occurring under hyperbaric conditions; - Pulmonary (lungs), characterised by difficulty in breathing and pain within the chest, occurring when breathing elevated pressures of oxygen for extended periods;
- Ocular (retinopathic conditionsRetinopathyRetinopathy is a general term that refers to some form of non-inflammatory damage to the retina of the eye. Frequently, retinopathy is an ocular manifestation of systemic disease.-Pathophysiology:Causes of retinopathy are varied:...
), characterised by alterations to the eyes, occurring when breathing elevated pressures of oxygen for extended periods.
Central nervous system oxygen toxicity can cause seizures, brief periods of rigidity followed by convulsions and unconsciousness, and is of concern to divers who encounter greater than atmospheric pressures. Pulmonary oxygen toxicity results in damage to the lungs, causing pain and difficulty in breathing. Oxidative damage to the eye may lead to myopia or partial detachment of the retina
Retina
The vertebrate retina is a light-sensitive tissue lining the inner surface of the eye. The optics of the eye create an image of the visual world on the retina, which serves much the same function as the film in a camera. Light striking the retina initiates a cascade of chemical and electrical...
. Pulmonary and ocular damage are most likely to occur when supplemental oxygen is administered as part of a treatment, particularly to newborn infants, but are also a concern during hyperbaric oxygen therapy.
Oxidative damage may occur in any cell in the body but the effects on the three most susceptible organs will be the primary concern. It may also be implicated in red blood cell destruction (haemolysis
Hemolysis
Hemolysis —from the Greek meaning "blood" and meaning a "loosing", "setting free" or "releasing"—is the rupturing of erythrocytes and the release of their contents into surrounding fluid...
), damage to liver (hepatic), heart (myocardial), endocrine
Endocrine system
In physiology, the endocrine system is a system of glands, each of which secretes a type of hormone directly into the bloodstream to regulate the body. The endocrine system is in contrast to the exocrine system, which secretes its chemicals using ducts. It derives from the Greek words "endo"...
glands (adrenal
Adrenal gland
In mammals, the adrenal glands are endocrine glands that sit atop the kidneys; in humans, the right suprarenal gland is triangular shaped, while the left suprarenal gland is semilunar shaped...
, gonad
Gonad
The gonad is the organ that makes gametes. The gonads in males are the testes and the gonads in females are the ovaries. The product, gametes, are haploid germ cells. For example, spermatozoon and egg cells are gametes...
s, and thyroid
Thyroid
The thyroid gland or simply, the thyroid , in vertebrate anatomy, is one of the largest endocrine glands. The thyroid gland is found in the neck, below the thyroid cartilage...
), or kidneys (renal), and general damage to cells
Cell (biology)
The cell is the basic structural and functional unit of all known living organisms. It is the smallest unit of life that is classified as a living thing, and is often called the building block of life. The Alberts text discusses how the "cellular building blocks" move to shape developing embryos....
.
In unusual circumstances, effects on other tissues may be observed: it is suspected that during spaceflight, high oxygen concentrations may contribute to bone damage. Hyperoxia can also indirectly cause carbon dioxide narcosis
CO2 retention
CO2 retention is a pathophysiological process in which too little carbon dioxide is removed from the blood by the lungs. The end result is hypercapnia, an elevated level of carbon dioxide dissolved in the bloodstream. Various diseases may lead to this state; disturbed gas exchange may lead to...
in patients with lung ailments such as chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease
Chronic obstructive pulmonary disease , also known as chronic obstructive lung disease , chronic obstructive airway disease , chronic airflow limitation and chronic obstructive respiratory disease , is the co-occurrence of chronic bronchitis and emphysema, a pair of commonly co-existing diseases...
or with central respiratory depression. Oxygen toxicity is not associated with hyperventilation
Hyperventilation
Hyperventilation or overbreathing is the state of breathing faster or deeper than normal, causing excessive expulsion of circulating carbon dioxide. It can result from a psychological state such as a panic attack, from a physiological condition such as metabolic acidosis, can be brought about by...
, because breathing air at atmospheric pressure always has a partial pressure of oxygen (ppO2) of 0.21 bar (21,000 Pa) and the lower limit for toxicity is more than 0.3 bar (30,000 Pa).
Signs and symptoms
| Exposure (mins.) | Num. of Subjects | Symptoms |
|---|---|---|
| 96 | 1 | Prolonged dazzle; severe spasmodic vomiting |
| 60–69 | 3 | Severe lip-twitching; Euphoria; Nausea and vertigo; arm twitch |
| 50–55 | 4 | Severe lip-twitching; Dazzle; Blubbering of lips; fell asleep; Dazed |
| 31–35 | 4 | Nausea, vertigo, lip-twitching; Convulsed |
| 21–30 | 6 | Convulsed; Drowsiness; Severe lip-twitching; epigastric aura; twitch L arm; amnesia |
| 16–20 | 8 | Convulsed; Vertigo and severe lip twitching; epigastric aura; spasmodic respiration; |
| 11–15 | 4 | Inspiratory predominance; lip-twitching and syncope; Nausea and confusion |
| 6–10 | 6 | Dazed and lip-twitching; paraesthesiae; vertigo; "Diaphragmatic spasm"; Severe nausea |
Central nervous system
Central nervous systemCentral nervous system
The central nervous system is the part of the nervous system that integrates the information that it receives from, and coordinates the activity of, all parts of the bodies of bilaterian animals—that is, all multicellular animals except sponges and radially symmetric animals such as jellyfish...
oxygen toxicity manifests as symptoms such as visual changes (especially tunnel vision
Tunnel vision
Tunnel vision is the loss of peripheral vision with retention of central vision, resulting in a constricted circular tunnel-like field of vision.- Medical / biological causes :Tunnel vision can be caused by:...
), ringing in the ears (tinnitus
Tinnitus
Tinnitus |ringing]]") is the perception of sound within the human ear in the absence of corresponding external sound.Tinnitus is not a disease, but a symptom that can result from a wide range of underlying causes: abnormally loud sounds in the ear canal for even the briefest period , ear...
), nausea
Nausea
Nausea , is a sensation of unease and discomfort in the upper stomach with an involuntary urge to vomit. It often, but not always, precedes vomiting...
, twitching (especially of the face), irritability (personality changes, anxiety
Anxiety
Anxiety is a psychological and physiological state characterized by somatic, emotional, cognitive, and behavioral components. The root meaning of the word anxiety is 'to vex or trouble'; in either presence or absence of psychological stress, anxiety can create feelings of fear, worry, uneasiness,...
, confusion, etc.), and dizziness
Vertigo (medical)
Vertigo is a type of dizziness, where there is a feeling of motion when one is stationary. The symptoms are due to a dysfunction of the vestibular system in the inner ear...
. This may be followed by a tonic–clonic seizure consisting of two phases: intense muscle contraction occurs for several seconds (tonic); followed by rapid spasms of alternate muscle relaxation and contraction producing convulsive jerking (clonic). The seizure ends with a period of unconsciousness (the postictal state
Postictal state
The postictal state is the altered state of consciousness that a person enters after experiencing a seizure. It usually lasts between 5 and 30 minutes, but sometimes longer in the case of larger or more severe seizures and is characterized by drowsiness, confusion, nausea, hypertension, headache or...
). The onset of seizure depends upon the partial pressure of oxygen (ppO2) in the breathing gas
Breathing gas
Breathing gas is a mixture of gaseous chemical elements and compounds used for respiration.Air is the most common and only natural breathing gas...
and exposure duration. However, exposure time before onset is unpredictable, as tests have shown a wide variation, both amongst individuals, and in the same individual from day to day.
In addition, many external factors, such as underwater immersion, exposure to cold, and exercise will decrease the time to onset of central nervous system symptoms.
Decrease of tolerance is closely linked to retention of carbon dioxide
Carbon dioxide
Carbon dioxide is a naturally occurring chemical compound composed of two oxygen atoms covalently bonded to a single carbon atom...
. Other factors, such as darkness and caffeine
Caffeine
Caffeine is a bitter, white crystalline xanthine alkaloid that acts as a stimulant drug. Caffeine is found in varying quantities in the seeds, leaves, and fruit of some plants, where it acts as a natural pesticide that paralyzes and kills certain insects feeding on the plants...
, increase tolerance in test animals, but these effects have not been proven in humans.
Pulmonary
Pulmonary toxicity symptoms result from an inflammation that starts in the airways leading to the lungs and then spreads into the lungs (tracheobronchial treeTracheobronchial tree
The tracheobronchial tree is the structure from the trachea, bronchi, and bronchioles that forms the airways that supply air to the lungs. It is within the neck and the chest. The structure looks like a tree because the trachea splits into the right and left mainstem bronchi, which "branch" into...
). The symptoms appear in the upper chest region (substernal and carinal
Carina of trachea
In anatomy, the carina is a cartilaginous ridge within the trachea that runs anteroposteriorly between the two primary bronchi at the site of the tracheal bifurcation at the lower end of the trachea .The mucous membrane of the carina is the most sensitive area of the trachea and larynx...
regions).
This begins as a mild tickle on inhalation and progresses to frequent coughing. If breathing elevated partial pressures of oxygen is not discontinued, patients experience a mild burning on inhalation along with uncontrollable coughing and occasional shortness of breath (dyspnoea
Dyspnea
Dyspnea , shortness of breath , or air hunger, is the subjective symptom of breathlessness.It is a normal symptom of heavy exertion but becomes pathological if it occurs in unexpected situations...
). Physical findings related to pulmonary toxicity have included bubbling sounds heard through a stethoscope
Stethoscope
The stethoscope is an acoustic medical device for auscultation, or listening to the internal sounds of an animal body. It is often used to listen to lung and heart sounds. It is also used to listen to intestines and blood flow in arteries and veins...
(bubbling rales
Rales
Crackles, crepitations, or rales are the clicking, rattling, or crackling noises that may be made by one or both lungs of a human with a respiratory disease during inhalation. They are often heard only with a stethoscope...
), fever, and increased blood flow to the lining of the nose (hyperaemia
Hyperaemia
Hyperaemia or hyperemia describes the increase of blood flow to different tissues in the body. It can have medical implications, but is also a regulatory response, allowing change in blood supply to different tissues through vasodilation. Clinically, hyperaemia in tissues manifest as erythema,...
of the nasal mucosa). The radiological finding from the lungs shows inflammation
Inflammation
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
and swelling (pulmonary oedema
Pulmonary edema
Pulmonary edema , or oedema , is fluid accumulation in the air spaces and parenchyma of the lungs. It leads to impaired gas exchange and may cause respiratory failure...
). Pulmonary function measurements
Spirometry
Spirometry is the most common of the pulmonary function tests , measuring lung function, specifically the measurement of the amount and/or speed of air that can be inhaled and exhaled...
are reduced, as noted by a reduction in the amount of air that the lungs can hold (vital capacity
Vital capacity
Vital capacity is the maximum amount of air a person can expel from the lungs after a maximum inspiration. It is equal to the inspiratory reserve volume plus the tidal volume plus the expiratory reserve volume....
) and changes in expiratory function and lung elasticity. Tests in animals have indicated a variation in tolerance similar to that found in central nervous system toxicity, as well as significant variations between species. When the exposure to oxygen above 0.5 bar (50,000 Pa) is intermittent, it permits the lungs to recover and delays the onset of toxicity.
Ocular
In premature babies, signs of damage to the eye (retinopathy of prematurityRetinopathy of prematurity
Retinopathy of prematurity , previously known as retrolental fibroplasia , is an eye disease that affects prematurely-born babies. It is thought to be caused by disorganized growth of retinal blood vessels which may result in scarring and retinal detachment. ROP can be mild and may resolve...
, or ROP) are observed via an ophthalmoscope as a demarcation between the vascularised and non-vascularised regions of an infant's retina. The degree of this demarcation is used to designate four stages: (I) the demarcation is a line; (II) the demarcation becomes a ridge; (III) growth of new blood vessels occurs around the ridge; (IV) the retina begins to detach from the inner wall of the eye (choroid
Choroid
The choroid, also known as the choroidea or choroid coat, is the vascular layer of the eye, containing connective tissue, and lying between the retina and the sclera. The human choroid is thickest at the far extreme rear of the eye , while in the outlying areas it narrows to 0.1 mm...
).
Causes
Oxygen toxicity is caused by exposure to oxygen at partial pressures greater than those to which the body is normally exposed. This occurs in three principal settings: underwater diving, hyperbaric oxygen therapy and the provision of supplemental oxygen, particularly to premature infants. In each case, the risk factorsRisk factors
A risk factor is a concept in finance theory such as the CAPM, APT and other theories that use pricing kernels. In these models, the rate of return of an asset is a random variable whose realization in any time period is a linear combination of other random variables plus a disturbance term or...
are markedly different.
Central nervous system toxicity
Exposures, from minutes to a few hours, to partial pressures of oxygen above 1.6 bars (160,000 Pa)—about eight times the atmospheric concentration—are usually associated with central nervous system oxygen toxicity and are most likely to occur among patients undergoing hyperbaric oxygen therapy and divers. Since atmospheric pressure is about 1 bars (100,000 Pa), central nervous system toxicity can only occur under hyperbaric conditions, where ambient pressureAmbient pressure
The ambient pressure on an object is the pressure of the surrounding medium, such as a gas or liquid, which comes into contact with the object....
is above normal. Divers breathing air at depths greater than 60 m (196.9 ft) face an increasing risk of an oxygen toxicity "hit" (seizure). Divers breathing a gas mixture enriched with oxygen, such as nitrox, can similarly suffer a seizure at shallower depths, should they descend below the maximum depth allowed for the mixture.
Pulmonary toxicity
The lungs, as well as the remainder of the respiratory tractRespiratory tract
In humans the respiratory tract is the part of the anatomy involved with the process of respiration.The respiratory tract is divided into 3 segments:*Upper respiratory tract: nose and nasal passages, paranasal sinuses, and throat or pharynx...
, are exposed to the highest concentration of oxygen in the human body and are therefore the first organs to show toxicity. Pulmonary toxicity occurs with exposure to concentrations of oxygen greater than 0.5 bar (50,000 Pa), corresponding to an oxygen fraction of 50% at normal atmospheric pressure. Signs of pulmonary toxicity begins with evidence of tracheobronchitis, or inflammation of the upper airways, after an asymptomatic period between 4 and 22 hours at greater than 95% oxygen, with some studies suggesting symptoms usually begin after approximately 14 hours at this level of oxygen.
At partial pressures of oxygen of 2 bar—100% oxygen at 2 to 3 times atmospheric pressure—these symptoms may begin as early as 3 hours after exposure to oxygen. Experiments on rats show pulmonary manifestations of oxygen toxicity are not the same for normobaric conditions as they are for hyperbaric conditions. Evidence of decline in lung function as measured by pulmonary function testing can occur as quickly as 24 hours of continuous exposure to 100% oxygen, with evidence of diffuse alveolar damage
Diffuse alveolar damage
Diffuse alveolar damage is a histological pattern in lung disease. It is seen in acute respiratory distress syndrome , transfusion related acute lung injury and acute interstitial pneumonia .-Prevalence:...
and the onset of acute respiratory distress syndrome
Acute respiratory distress syndrome
Acute respiratory distress syndrome , also known as respiratory distress syndrome or adult respiratory distress syndrome is a serious reaction to various forms of injuries to the lung....
usually occurring after 48 hours on 100% oxygen. Breathing 100% oxygen also eventually leads to collapse of the alveoli (atelectasis
Atelectasis
Atelectasis is defined as the collapse or closure of alveoli resulting in reduced or absent gas exchange. It may affect part or all of one lung. It is a condition where the alveoli are deflated, as distinct from pulmonary consolidation.It is a very common finding in chest x-rays and other...
), while—at the same partial pressure of oxygen—the presence of significant partial pressures of inert gases, typically nitrogen, will prevent this effect.
Preterm newborns are known to be at higher risk for bronchopulmonary dysplasia
Bronchopulmonary dysplasia
Bronchopulmonary dysplasia is a chronic lung disorder that is most common among children who were born prematurely, with low birthweights and who received prolonged mechanical ventilation to treat respiratory distress syndrome...
with extended exposure to high concentrations of oxygen. Other groups at higher risk for oxygen toxicity are patients on mechanical ventilation
Mechanical ventilation
In medicine, mechanical ventilation is a method to mechanically assist or replace spontaneous breathing. This may involve a machine called a ventilator or the breathing may be assisted by a physician, respiratory therapist or other suitable person compressing a bag or set of bellows...
with exposure to levels of oxygen greater than 50%, and patients exposed to chemicals that increase risk for oxygen toxicity such the chemotherapeutic agent bleomycin
Bleomycin
Bleomycin is a glycopeptide antibiotic produced by the bacterium Streptomyces verticillus. Bleomycin refers to a family of structurally related compounds. When used as an anticancer agent, the chemotherapeutical forms are primarily bleomycin A2 and B2. It works by causing breaks in DNA...
. Therefore, current guidelines for patients on mechanical ventilation in intensive care suggests keeping oxygen concentration less than 60%. Likewise, divers who undergo treatment of decompression sickness
Decompression sickness
Decompression sickness describes a condition arising from dissolved gases coming out of solution into bubbles inside the body on depressurization...
are at increased risk of oxygen toxicity as treatment entails exposure to long periods of oxygen breathing under hyperbaric conditions, in addition to any oxygen exposure during the dive.
Ocular toxicity
Prolonged exposure to high inspired fractions of oxygen causes damage to the retinaRetina
The vertebrate retina is a light-sensitive tissue lining the inner surface of the eye. The optics of the eye create an image of the visual world on the retina, which serves much the same function as the film in a camera. Light striking the retina initiates a cascade of chemical and electrical...
.
Damage to the developing eye of infants exposed to high oxygen fraction at normal pressure has a different mechanism and effect from the eye damage experienced by adult divers under hyperbaric conditions.
Hyperoxia may be a contributing factor for the disorder called retrolental fibroplasia or retinopathy of prematurity (ROP) in infants.
In preterm infants, the retina is often not fully vascularised. Retinopathy of prematurity occurs when the development of the retinal vasculature is arrested and then proceeds abnormally. Associated with the growth of these new vessels is fibrous tissue
Granulation tissue
Granulation tissue is the perfused, fibrous connective tissue that replaces a fibrin clot in healing wounds. Granulation tissue typically grows from the base of a wound and is able to fill wounds of almost any size it heals...
(scar tissue) that may contract to cause retinal detachment. Supplemental oxygen exposure, while a risk factor
Risk factor
In epidemiology, a risk factor is a variable associated with an increased risk of disease or infection. Sometimes, determinant is also used, being a variable associated with either increased or decreased risk.-Correlation vs causation:...
, is not the main risk factor for development of this disease. Restricting supplemental oxygen use does not necessarily reduce the rate of retinopathy of prematurity, and may raise the risk of hypoxia-related systemic complications.
Hyperoxic myopia
Myopia
Myopia , "shortsightedness" ) is a refractive defect of the eye in which collimated light produces image focus in front of the retina under conditions of accommodation. In simpler terms, myopia is a condition of the eye where the light that comes in does not directly focus on the retina but in...
has occurred in closed circuit oxygen rebreather divers with prolonged exposures.
It also occurs frequently in those undergoing repeated hyperbaric oxygen therapy. This is due to an increase in the refractive power of the lens
Lens (anatomy)
The crystalline lens is a transparent, biconvex structure in the eye that, along with the cornea, helps to refract light to be focused on the retina. The lens, by changing shape, functions to change the focal distance of the eye so that it can focus on objects at various distances, thus allowing a...
, since axial length and keratometry
Keratometer
A keratometer, also known as a ophthalmometer, is a diagnostic instrument for measuring the curvature of the anterior surface of the cornea, particularly for assessing the extent and axis of astigmatism...
readings do not reveal a cornea
Cornea
The cornea is the transparent front part of the eye that covers the iris, pupil, and anterior chamber. Together with the lens, the cornea refracts light, with the cornea accounting for approximately two-thirds of the eye's total optical power. In humans, the refractive power of the cornea is...
l or length basis for a myopic shift. It is usually reversible with time.
Mechanism
Metabolism
Metabolism is the set of chemical reactions that happen in the cells of living organisms to sustain life. These processes allow organisms to grow and reproduce, maintain their structures, and respond to their environments. Metabolism is usually divided into two categories...
of oxygen and have important roles in cell signalling.
One species produced by the body, the superoxide
Superoxide
A superoxide, also known by the obsolete name hyperoxide, is a compound that possesses the superoxide anion with the chemical formula O2−. The systematic name of the anion is dioxide. It is important as the product of the one-electron reduction of dioxygen O2, which occurs widely in nature...
anion (O2–), is possibly involved in iron acquisition.
Higher than normal concentrations of oxygen lead to increased levels of reactive oxygen species.
Oxygen is necessary for cell metabolism, and the blood supplies it to all parts of the body. When oxygen is breathed at high partial pressures, a hyperoxic condition will rapidly spread, with the most vascularised tissues being most vulnerable.
During times of environmental stress, levels of reactive oxygen species can increase dramatically, which can damage cell structures and produce oxidative stress
Oxidative stress
Oxidative stress represents an imbalance between the production and manifestation of reactive oxygen species and a biological system's ability to readily detoxify the reactive intermediates or to repair the resulting damage...
.
While all the reaction mechanisms of these species within the body are not yet fully understood,
one of the most reactive products of oxidative stress is the hydroxyl radical
Hydroxyl radical
The hydroxyl radical, •OH, is the neutral form of the hydroxide ion . Hydroxyl radicals are highly reactive and consequently short-lived; however, they form an important part of radical chemistry. Most notably hydroxyl radicals are produced from the decomposition of hydroperoxides or, in...
(·OH), which can initiate a damaging chain reaction of lipid peroxidation
Lipid peroxidation
Lipid peroxidation refers to the oxidative degradation of lipids. It is the process in which free radicals "steal" electrons from the lipids in cell membranes, resulting in cell damage. This process proceeds by a free radical chain reaction mechanism...
in the unsaturated lipids within cell membranes.
High concentrations of oxygen also increase the formation of other free radicals, such as nitric oxide
Nitric oxide
Nitric oxide, also known as nitrogen monoxide, is a diatomic molecule with chemical formula NO. It is a free radical and is an important intermediate in the chemical industry...
, peroxynitrite
Peroxynitrite
Peroxynitrite is the anion with the formula ONOO−. It is an unstable structural isomer of nitrate, NO3−, which has the same formula but a different structure. Although peroxynitrous acid is highly reactive, its conjugate base peroxynitrite is stable in basic solution...
, and trioxidane
Trioxidane
Trioxidane, hydrogen trioxide or dihydrogen trioxide is an unstable molecule with the formula H2O3 or HOOOH. It is one of the hydrogen polyoxides. In aqueous solutions, trioxidane decomposes to form water and singlet oxygen:...
, which harm DNA
DNA
Deoxyribonucleic acid is a nucleic acid that contains the genetic instructions used in the development and functioning of all known living organisms . The DNA segments that carry this genetic information are called genes, but other DNA sequences have structural purposes, or are involved in...
and other biomolecules.
Although the body has many antioxidant
Antioxidant
An antioxidant is a molecule capable of inhibiting the oxidation of other molecules. Oxidation is a chemical reaction that transfers electrons or hydrogen from a substance to an oxidizing agent. Oxidation reactions can produce free radicals. In turn, these radicals can start chain reactions. When...
systems such as glutathione
Glutathione
Glutathione is a tripeptide that contains an unusual peptide linkage between the amine group of cysteine and the carboxyl group of the glutamate side-chain...
that guard against oxidative stress, these systems are eventually overwhelmed at very high concentrations of free oxygen, and the rate of cell damage exceeds the capacity of the systems that prevent or repair it. Cell damage and cell death then result.
Diagnosis
Diagnosis of central nervous system oxygen toxicity in divers prior to seizure is difficult as the symptoms of visual disturbance, ear problems, dizziness, confusion and nausea can be due to many factors common to the underwater environment such as narcosisNitrogen narcosis
Narcosis while diving , is a reversible alteration in consciousness that occurs while scuba diving at depth. The Greek word ναρκωσις is derived from narke, "temporary decline or loss of senses and movement, numbness", a term used by Homer and Hippocrates...
, congestion and coldness. However, these symptoms may be helpful in diagnosing the first stages of oxygen toxicity in patients undergoing hyperbaric oxygen therapy. In either case, unless there is a prior history of epilepsy
Epilepsy
Epilepsy is a common chronic neurological disorder characterized by seizures. These seizures are transient signs and/or symptoms of abnormal, excessive or hypersynchronous neuronal activity in the brain.About 50 million people worldwide have epilepsy, and nearly two out of every three new cases...
or tests indicate hypoglycaemia
Hypoglycemia
Hypoglycemia or hypoglycæmia is the medical term for a state produced by a lower than normal level of blood glucose. The term literally means "under-sweet blood"...
, a seizure occurring in the setting of breathing oxygen at partial pressures greater than 1.4 bar (140,000 Pa) suggests a diagnosis of oxygen toxicity.
Diagnosis of bronchopulmonary dysplasia in new-born infants with breathing difficulties is difficult in the first few weeks. However, if the infant's breathing does not improve during this time, blood tests and x-rays may be used to confirm bronchopulmonary dysplasia. In addition, an echocardiogram can help to eliminate other possible causes such as congenital heart defects or pulmonary arterial hypertension.
The diagnosis of retinopathy of prematurity in infants is typically suggested by the clinical setting. Prematurity, low birth weight and a history of oxygen exposure are the principal indicators, while no hereditary factors have been shown to yield a pattern.
Prevention
Underwater
A seizure caused by oxygen toxicity to the central nervous system is a deadly but avoidable event while divingUnderwater diving
Underwater diving is the practice of going underwater, either with breathing apparatus or by breath-holding .Recreational diving is a popular activity...
. The diver may experience no warning symptoms. The effects are sudden convulsions and unconsciousness, during which victims can lose their regulator
Diving regulator
A diving regulator is a pressure regulator used in scuba or surface supplied diving equipment that reduces pressurized breathing gas to ambient pressure and delivers it to the diver. The gas may be air or one of a variety of specially blended breathing gases...
and drown. One of the advantages of a full-face diving mask is prevention of regulator loss in the event of a seizure. As there is an increased risk of central nervous system oxygen toxicity on deep dives, long dives and dives where oxygen-rich breathing gases are used, divers are taught to calculate a maximum operating depth
Maximum operating depth
In technical diving and nitrox diving, the maximum operating depth of a breathing gas is the depth at which the partial pressure of oxygen of the gas mix exceeds a safe limit...
for oxygen-rich breathing gas
Breathing gas
Breathing gas is a mixture of gaseous chemical elements and compounds used for respiration.Air is the most common and only natural breathing gas...
es, and cylinders containing such mixtures must be clearly marked with that depth.
In some diver training
Diver training
Diver training is the process of developing skills and building experience in the use of diving equipment and techniques so that the diver is able to dive safely and have fun....
courses for these types of diving, divers are taught to plan and monitor what is called the oxygen clock of their dives. This is a notional alarm clock, which ticks more quickly at increased ppO2 and is set to activate at the maximum single exposure limit recommended in the National Oceanic and Atmospheric Administration
National Oceanic and Atmospheric Administration
The National Oceanic and Atmospheric Administration , pronounced , like "noah", is a scientific agency within the United States Department of Commerce focused on the conditions of the oceans and the atmosphere...
Diving Manual. For the following partial pressures of oxygen the limit is: 45 minutes at 1.6 bar (160,000 Pa), 120 minutes at 1.5 bar (150,000 Pa), 150 minutes at 1.4 bar (140,000 Pa), 180 minutes at 1.3 bar (130,000 Pa) and 210 minutes at 1.2 bar (120,000 Pa), but is impossible to predict with any reliability whether or when toxicity symptoms will occur.
Many nitrox-capable dive computer
Dive computer
A dive computer or decompression meter is a device used by a scuba diver to measure the time and depth of a dive so that a safe ascent profile can be calculated and displayed so that the diver can avoid decompression sickness.- Purpose :...
s calculate an oxygen loading and can track it across multiple dives. The aim is to avoid activating the alarm by reducing the ppO2 of the breathing gas or the length of time breathing gas of higher ppO2. As the ppO2 depends on the fraction of oxygen in the breathing gas and the depth of the dive, the diver obtains more time on the oxygen clock by diving at a shallower depth, by breathing a less oxygen-rich gas, or by shortening the duration of exposure to oxygen-rich gases.
Diving below 60 m (196.9 ft) on air would expose a diver to increasing danger of oxygen toxicity as the partial pressure of oxygen exceeds 1.4 bar (140,000 Pa), so a gas mixture must be used which contains less than 21% oxygen (a hypoxic mixture). Increasing the proportion of nitrogen
Nitrogen
Nitrogen is a chemical element that has the symbol N, atomic number of 7 and atomic mass 14.00674 u. Elemental nitrogen is a colorless, odorless, tasteless, and mostly inert diatomic gas at standard conditions, constituting 78.08% by volume of Earth's atmosphere...
is not viable, since it would produce a strongly narcotic
Nitrogen narcosis
Narcosis while diving , is a reversible alteration in consciousness that occurs while scuba diving at depth. The Greek word ναρκωσις is derived from narke, "temporary decline or loss of senses and movement, numbness", a term used by Homer and Hippocrates...
mixture. However, helium
Helium
Helium is the chemical element with atomic number 2 and an atomic weight of 4.002602, which is represented by the symbol He. It is a colorless, odorless, tasteless, non-toxic, inert, monatomic gas that heads the noble gas group in the periodic table...
is not narcotic, and a usable mixture may be blended
Gas blending
Gas blending or gas mixing is the filling of diving cylinders with non-air breathing gases such as nitrox, trimix and heliox.Filling cylinders with a mixture of gases has dangers for both the filler and the diver. During filling there is a risk of fire due to use of oxygen and a risk of explosion...
either by completely replacing nitrogen with helium (the resulting mix is called heliox
Heliox
Heliox is a breathing gas composed of a mixture of helium and oxygen .Heliox has been used medically since the 1930s, and although the medical community adopted it initially to alleviate symptoms of upper airway obstruction, its range of medical uses has since expanded greatly, mostly because of...
), or by replacing part of the nitrogen with helium, producing a trimix.
Pulmonary oxygen toxicity is an entirely avoidable event while diving. The limited duration and naturally intermittent nature of most diving makes this a relatively rare (and even then, reversible) complication for divers. Guidelines have been established that allow divers to calculate when they are at risk of pulmonary toxicity.
Hyperbaric setting
The presence of a fever or a history of seizure is a relative contraindication to hyperbaric oxygen treatment. The schedules used for treatment of decompression illnessDecompression illness
Decompression Illness describes a collection of symptoms arising from decompression of the body.DCI is caused by two different mechanisms, which result in overlapping sets of symptoms. The two mechanisms are:...
allow for periods of breathing air rather than 100% oxygen (oxygen breaks) to reduce the chance of seizure or lung damage. The U.S. Navy uses treatment tables based on periods alternating between 100% oxygen and air. For example, U.S.N. table 6 requires 75 minutes (three periods of 20 minutes oxygen/5 minutes air) at an ambient pressure of 2.8 standard atmospheres (283,710 Pa), equivalent to a depth of 18 metres (59.1 ft). This is followed by a slow reduction in pressure to 1.9 atm (192,517.5 Pa) over 30 minutes on oxygen. The patient then remains at that pressure for a further 150 minutes, consisting of two periods of 15 minutes air/60 minutes oxygen, before the pressure is reduced to atmospheric over 30 minutes on oxygen.
Vitamin E
Vitamin E
Vitamin E is used to refer to a group of fat-soluble compounds that include both tocopherols and tocotrienols. There are many different forms of vitamin E, of which γ-tocopherol is the most common in the North American diet. γ-Tocopherol can be found in corn oil, soybean oil, margarine and dressings...
and selenium
Selenium
Selenium is a chemical element with atomic number 34, chemical symbol Se, and an atomic mass of 78.96. It is a nonmetal, whose properties are intermediate between those of adjacent chalcogen elements sulfur and tellurium...
were proposed and later rejected as a potential method of protection against pulmonary oxygen toxicity.
There is however some experimental evidence in rats that vitamin E and selenium aid in preventing in vivo
In vivo
In vivo is experimentation using a whole, living organism as opposed to a partial or dead organism, or an in vitro controlled environment. Animal testing and clinical trials are two forms of in vivo research...
lipid peroxidation
Lipid peroxidation
Lipid peroxidation refers to the oxidative degradation of lipids. It is the process in which free radicals "steal" electrons from the lipids in cell membranes, resulting in cell damage. This process proceeds by a free radical chain reaction mechanism...
and free radical damage, and therefore prevent retinal changes following repetitive hyperbaric oxygen exposures.
Normobaric setting
Bronchopulmonary dysplasia is reversible in the early stages by use of break periods on lower pressures of oxygen, but it may eventually result in irreversible lung injury if allowed to progress to severe damage. One or two days of exposure without oxygen breaks are needed to cause such damage.Retinopathy of prematurity is largely preventable by screening. Current guidelines require that all babies of less than 32 weeks gestational age
Gestational age
Gestational age relates to the age of an embryo or fetus . There is some ambiguity in how it is defined:*In embryology, gestational age is the time elapsed since conception. This interval is also termed fertilisation age....
or having a birth weight less than 1.5 kg (3.3 lb) should be screened for retinopathy of prematurity at least every two weeks.
The National Cooperative Study in 1954 showed a causal link between supplemental oxygen and retinopathy of prematurity, but subsequent curtailment of supplemental oxygen caused an increase in infant mortality. To balance the risks of hypoxia
Hypoxia (medical)
Hypoxia, or hypoxiation, is a pathological condition in which the body as a whole or a region of the body is deprived of adequate oxygen supply. Variations in arterial oxygen concentrations can be part of the normal physiology, for example, during strenuous physical exercise...
and retinopathy of prematurity, modern protocols now require monitoring of blood oxygen levels in premature infants receiving oxygen.
Hypobaric setting
In low-pressure environments oxygen toxicity may be avoided since the toxicity is caused by high partial pressure of oxygen, not merely by high oxygen fraction. This is illustrated by modern pure oxygen use in spacesuits, which must operate at low pressure (also historically, very high percentage oxygen and lower than normal atmospheric pressure was used in early spacecraft, for example, the GeminiProject Gemini
Project Gemini was the second human spaceflight program of NASA, the civilian space agency of the United States government. Project Gemini was conducted between projects Mercury and Apollo, with ten manned flights occurring in 1965 and 1966....
and Apollo spacecraft
Apollo spacecraft
The Apollo spacecraft was composed of five combined parts designed to accomplish the American Apollo program's goal of landing astronauts on the Moon by the end of the 1960s and returning them safely to Earth...
).
In such applications as extra-vehicular activity
Extra-vehicular activity
Extra-vehicular activity is work done by an astronaut away from the Earth, and outside of a spacecraft. The term most commonly applies to an EVA made outside a craft orbiting Earth , but also applies to an EVA made on the surface of the Moon...
, high-fraction oxygen is non-toxic, even at breathing mixture fractions approaching 100%, because the oxygen partial pressure is not allowed to chronically
Chronic toxicity
Chronic toxicity is a property of a substance that has toxic effects on a living organism, when that organism is exposed to the substance continuously or repeatedly. Compared with acute toxicity.Two distinct situations need to be considered:...
exceed 0.3 bar (4.4 psi).
Management
A seizure underwater requires that the diver is brought to the surface as soon as practicable. Although for many years the recommendation has been not to raise the diver during the seizure itself, owing to the danger of arterial gas embolism, there is no evidence of expiratory obstruction during seizure and benefit may be gained by raising the diver during the seizure's clonic phase.
Rescuers need to ensure that their own safety is not compromised during the convulsive phase. They then ensure that the victim's air supply is established and maintained, and carry out a controlled buoyant lift
Controlled buoyant lift
The controlled buoyant lift is an underwater diver rescue technique used by scuba divers to safely raise an incapacitated diver to the surface from depth. It is the primary technique for rescuing an underwater and unconscious diver...
. Lifting an unconscious body is taught by most diver training
Diver training
Diver training is the process of developing skills and building experience in the use of diving equipment and techniques so that the diver is able to dive safely and have fun....
agencies. Upon reaching the surface, emergency services are always contacted as there is a possibility of further complications requiring medical attention. The U.S. Navy has procedures for completing the decompression stops where a recompression chamber is not immediately available.
The occurrence of symptoms of bronchopulmonary dysplasia or acute respiratory distress syndrome is treated by lowering the fraction of oxygen administered, along with a reduction in the periods of exposure and an increase in the break periods where normal air is supplied. Where supplemental oxygen is required for treatment of another disease (particularly in infants), a ventilator may be needed to ensure that the lung tissue remains inflated. Reductions in pressure and exposure will be made progressively and medications such as bronchodilators and pulmonary surfactant
Pulmonary surfactant
Pulmonary surfactant is a surface-active lipoprotein complex formed by type II alveolar cells. The proteins and lipids that surfactant comprises have both a hydrophilic region and a hydrophobic region...
s may be used.
Retinopathy of prematurity may regress
Regression (medicine)
Regression in medicine is a characteristic of diseases to show lighter symptoms without completely disappearing. At a later point, symptoms may return. These symptoms are then called recidive....
spontaneously, but should the disease progress beyond a threshold (defined as five contiguous or eight cumulative hours of stage 3 retinopathy of prematurity), both cryosurgery
Cryosurgery
Cryosurgery is the application of extreme cold to destroy abnormal or diseased tissue. The term comes from the Greek words cryo and surgery meaning "hand work" or "handiwork"....
and laser surgery
Laser surgery
Laser surgery is surgery using a laser to cut tissue instead of a scalpel. Examples include the use of a laser scalpel in otherwise conventional surgery, and soft tissue laser surgery, in which the laser beam vaporizes soft tissue with high water content...
have been shown to reduce the risk of blindness as an outcome. Where the disease has progressed further, techniques such as scleral buckling
Scleral buckle
A scleral buckle is one of several ophthalmologic procedures that can be used to repair a retinal detachment. Retinal detachments are usually caused by retinal tears, and a scleral buckle can be used to close the retinal break....
and vitrectomy
Vitrectomy
Vitrectomy is a surgery to remove some or all of the vitreous humor from the eye. Anterior vitrectomy entails removing small portions of the vitreous from the front structures of the eye—often because these are tangled in an intraocular lens or other structures...
surgery may assist in re-attaching the retina.
Prognosis
Although the convulsions caused by central nervous system oxygen toxicity may lead to incidental injury to the victim, it remained uncertain for many years whether damage to the nervous system following the seizure could occur and several studies searched for evidence of such damage. An overview of these studies by Bitterman in 2004 concluded that following removal of breathing gas containing high fractions of oxygen, no long-term neurological damage from the seizure remains.The majority of infants who have survived following an incidence of bronchopulmonary dysplasia will eventually recover near-normal lung function, since lungs continue to grow during the first 5–7 years and the damage caused by bronchopulmonary dysplasia is to some extent reversible (even in adults). However, they are likely be more susceptible to respiratory infections for the rest of their lives and the severity of later infections is often greater than that in their peers.
Retinopathy of prematurity (ROP) in infants frequently regresses without intervention and eyesight may be normal in later years. Where the disease has progressed to the stages requiring surgery, the outcomes are generally good for the treatment of stage 3 ROP, but are much worse for the later stages. Although surgery is usually successful in restoring the anatomy of the eye, damage to the nervous system by the progression of the disease leads to comparatively poorer results in restoring vision. The presence of other complicating diseases also reduces the likelihood of a favourable outcome.
Epidemiology
The incidence of central nervous system toxicity among divers has decreased since the Second World War, as protocols have developed to limit exposure and partial pressure of oxygen inspired. In 1947, Donald recommended limiting the depth allowed for breathing pure oxygen to 7.6 m (24.9 ft), or a ppO2 of 1.8 bar (180,000 Pa). This limit has been reduced, until today a limit of 1.4 bar (140,000 Pa) during a recreational dive and 1.6 bar (160,000 Pa) during shallow decompression stops is accepted. Oxygen toxicity has now become a rare occurrence other than when caused by equipment malfunction and human error. Historically, the U.S. Navy has refined its Navy Diving Manual Tables to reduce oxygen toxicity incidents. Between 1995 and 1999, reports showed 405 surface-supported dives using the helium–oxygen tables; of these, oxygen toxicity symptoms were observed on 6 dives (1.5%). As a result, the U.S. Navy in 2000 modified the schedules and conducted field tests of 150 dives, none of which produced symptoms of oxygen toxicity. Revised tables were published in 2001.The variability in tolerance and other variable factors such as workload have resulted in the U.S. Navy abandoning screening for oxygen tolerance. Of the 6,250 oxygen-tolerance tests performed between 1976 and 1997, only 6 episodes of oxygen toxicity were observed (0.1%).
Central nervous system oxygen toxicity among patients undergoing hyperbaric oxygen therapy is rare, and is influenced by a number of a factors: individual sensitivity and treatment protocol; and probably therapy indication
Indication (medicine)
In medicine, an indication is a valid reason to use a certain test, medication, procedure, or surgery. The opposite of indication is contraindication.-Drugs:...
and equipment used. A study by Welslau in 1996 reported 16 incidents out of a population of 107,264 patients (0.015%), while Hampson and Atik in 2003 found a rate of 0.03%. Yildiz, Ay and Qyrdedi, in a summary of 36,500 patient treatments between 1996 and 2003, reported only 3 oxygen toxicity incidents, giving a rate of 0.008%. A later review of over 80,000 patient treatments revealed an even lower rate: 0.0024%. The reduction in incidence may be partly due to use of a mask (rather than a hood) to deliver oxygen.
Bronchopulmonary dysplasia is among the most common complications of prematurely born
Premature birth
In humans preterm birth refers to the birth of a baby of less than 37 weeks gestational age. The cause for preterm birth is in many situations elusive and unknown; many factors appear to be associated with the development of preterm birth, making the reduction of preterm birth a challenging...
infants and its incidence has grown as the survival of extremely premature infants has increased. Nevertheless, the severity has decreased as better management of supplemental oxygen has resulted in the disease now being related mainly to factors other than hyperoxia.
In 1997 a summary of studies of neonatal intensive care units in industrialised countries showed that up to 60% of low birth weight
Low birth weight
Low birth weight is defined as a birth weight of a liveborn infant of less than 2,500 g. regardless of gestational age-Causes:LBW is either the result of preterm birth or of the infant being small for gestational age , or a combination of...
babies developed retinopathy of prematurity, which rose to 72% in extremely low birth weight babies, defined as less than 1 kg (2.2 lb) at birth. However, severe outcomes are much less frequent: for very low birth weight babies—those less than 1.5 kg (3.3 lb) at birth—the incidence of blindness was found to be no more than 8%.
History
Paul Bert
Paul Bert was a French zoologist, physiologist and politician. He is sometimes given the sobriquet "Father of Aviation Medicine".-Life:Bert was born at Auxerre...
in 1878.
He showed that oxygen was toxic to insects, arachnids, myriapods
Myriapoda
Myriapoda is a subphylum of arthropods containing millipedes, centipedes, and others. The group contains 13,000 species, all of which are terrestrial...
, molluscs, earthworms, fungi, germinating seeds, birds, and other animals. Central nervous system toxicity may be referred to as the "Paul Bert effect".
Pulmonary oxygen toxicity was first described by J. Lorrain Smith in 1899 when he noted central nervous system toxicity and discovered in experiments in mice and birds that 0.43 bar (43,000 Pa) had no effect but 0.75 bar (75,000 Pa) of oxygen was a pulmonary irritant.
Pulmonary toxicity may be referred to as the "Lorrain Smith effect".
The first recorded human exposure was undertaken in 1910 by Bornstein when two men breathed oxygen at 2.8 bar (280,000 Pa) for 30 minutes while he went on to 48 minutes with no symptoms. In 1912, Bornstein developed cramps in his hands and legs while breathing oxygen at 2.8 bar (280,000 Pa) for 51 minutes.
Smith then went on to show that intermittent exposure to a breathing gas with less oxygen permitted the lungs to recover and delayed the onset of pulmonary toxicity.
Albert R. Behnke
Albert R. Behnke
Captain Albert Richard Behnke Jr. USN was an American physician, who was principally responsible for developing the U.S. Naval Medical Research Institute...
et al. in 1935 were the first to observe visual field
Visual field
The term visual field is sometimes used as a synonym to field of view, though they do not designate the same thing. The visual field is the "spatial array of visual sensations available to observation in introspectionist psychological experiments", while 'field of view' "refers to the physical...
contraction (tunnel vision
Tunnel vision
Tunnel vision is the loss of peripheral vision with retention of central vision, resulting in a constricted circular tunnel-like field of vision.- Medical / biological causes :Tunnel vision can be caused by:...
) on dives between 1 bar (100,000 Pa) and 4.1 bar (410,000 Pa).
During World War II, Donald and Yarbrough et al. performed over 2,000 experiments on oxygen toxicity to support the initial use of closed circuit oxygen rebreather
Rebreather
A rebreather is a type of breathing set that provides a breathing gas containing oxygen and recycled exhaled gas. This recycling reduces the volume of breathing gas used, making a rebreather lighter and more compact than an open-circuit breathing set for the same duration in environments where...
s.
Naval divers in the early years of oxygen rebreather diving developed a mythology about a monster called "Oxygen Pete", who lurked in the bottom of the Admiralty Experimental Diving Unit "wet pot" (a water-filled hyperbaric chamber) to catch unwary divers. They called having an oxygen toxicity attack "getting a Pete".
In the decade following World War II, Lambertsen
Christian J. Lambertsen
Christian James Lambertsen was an American environmental medicine and diving medicine specialist who was principally responsible for developing the United States Navy frogmen's rebreathers in the early 1940s for underwater warfare...
et al. made further discoveries on the effects of breathing oxygen under pressure as well as methods of prevention.
Their work on intermittent exposures for extension of oxygen tolerance and on a model for prediction of pulmonary oxygen toxicity based on pulmonary function are key documents in the development of standard operating procedures when breathing elevated pressures of oxygen.
Lambertsen's work showing the effect of carbon dioxide in decreasing time to onset of central nervous system symptoms has influenced work from current exposure guidelines to future breathing apparatus
Scuba set
A scuba set is an independent breathing set that provides a scuba diver with the breathing gas necessary to breathe underwater during scuba diving. It is much used for sport diving and some sorts of work diving....
design.
Retinopathy of prematurity was not observed prior to World War II, but with the availability of supplemental oxygen in the decade following, it rapidly became one of the principal causes of infant blindness in developed countries. By 1960 the use of oxygen had become identified as a risk factor and its administration restricted. The resulting fall in retinopathy of prematurity was accompanied by a rise in infant mortality and hypoxia
Hypoxia (medical)
Hypoxia, or hypoxiation, is a pathological condition in which the body as a whole or a region of the body is deprived of adequate oxygen supply. Variations in arterial oxygen concentrations can be part of the normal physiology, for example, during strenuous physical exercise...
-related complications. Since then, more sophisticated monitoring and diagnosis have established protocols for oxygen use which aim to balance between hypoxic conditions and problems of retinopathy of prematurity.
Bronchopulmonary dysplasia was first described by Northway in 1967, who outlined the conditions that would lead to the diagnosis.
This was later expanded by Bancalari and in 1988 by Shennan, who suggested the need for supplemental oxygen at 36 weeks could predict long-term outcomes.
Nevertheless, Palta et al. in 1998 concluded that radiographic evidence was the most accurate predictor of long-term effects.
Bitterman et al. in 1986 and 1995 showed that darkness
Lighting
Lighting or illumination is the deliberate application of light to achieve some practical or aesthetic effect. Lighting includes the use of both artificial light sources such as lamps and light fixtures, as well as natural illumination by capturing daylight...
and caffeine
Caffeine
Caffeine is a bitter, white crystalline xanthine alkaloid that acts as a stimulant drug. Caffeine is found in varying quantities in the seeds, leaves, and fruit of some plants, where it acts as a natural pesticide that paralyzes and kills certain insects feeding on the plants...
would delay the onset of changes to brain electrical activity
Electroencephalography
Electroencephalography is the recording of electrical activity along the scalp. EEG measures voltage fluctuations resulting from ionic current flows within the neurons of the brain...
in rats.
In the years since, research on central nervous system toxicity has centred on methods of prevention and safe extension of tolerance.
Sensitivity to central nervous system oxygen toxicity has been shown to be affected by factors such as circadian rhythm
Circadian rhythm
A circadian rhythm, popularly referred to as body clock, is an endogenously driven , roughly 24-hour cycle in biochemical, physiological, or behavioural processes. Circadian rhythms have been widely observed in plants, animals, fungi and cyanobacteria...
, drugs, age, and gender.
In 1988, Hamilton et al. wrote procedures for the National Oceanic and Atmospheric Administration to establish oxygen exposure limits for habitat
Underwater habitat
Underwater habitats are underwater structures in which people can live for extended periods and carry out most of the basic human functions of a 24-hour day, such as working, resting, eating, attending to personal hygiene, and sleeping...
operations.
Even today, models for the prediction of pulmonary oxygen toxicity do not explain all the results of exposure to high partial pressures of oxygen.
Society and culture
Recreational scuba diversRecreational diving
Recreational diving or sport diving is a type of diving that uses SCUBA equipment for the purpose of leisure and enjoyment. In some diving circles, the term "recreational diving" is used in contradistinction to "technical diving", a more demanding aspect of the sport which requires greater levels...
commonly breathe nitrox containing up to 40% oxygen, while technical divers
Technical diving
Technical diving is a form of scuba diving that exceeds the scope of recreational diving...
use pure oxygen or nitrox containing up to 80% oxygen. Divers who breathe oxygen fractions greater than in air (21%) need to be trained in the dangers of oxygen toxicity and how to prevent them. In order to buy nitrox, a diver has to show evidence of such qualification.
Since the late 1990s the recreational use of oxygen has been promoted by oxygen bars, where customers breathe oxygen through a nasal cannula
Nasal cannula
The nasal cannula is a device used to deliver supplemental oxygen or airflow to a patient or person in need of respiratory help. This device consists of a plastic tube which fits behind the ears, and a set of two prongs which are placed in the nostrils. Oxygen flows from these prongs...
. Claims have been made that this reduces stress, increases energy, and lessens the effects of hangovers and headaches, despite the lack of any scientific evidence to support them.
There are also devices on sale that offer "oxygen massage" and "oxygen detoxification" with claims of removing body toxins and reducing body fat.
The American Lung Association
American Lung Association
The American Lung Association is a voluntary health organization whose mission is to save lives by improving lung health and preventing lung disease.-History:...
has stated "there is no evidence that oxygen at the low flow levels used in bars can be dangerous to a normal person's health", but the U.S. Center for Drug Evaluation and Research
Center for Drug Evaluation and Research
The Center for Drug Evaluation and Research is a division of the U.S. Food and Drug Administration that monitors most drugs as defined in the Food, Drug, and Cosmetic Act. Some biological products are also legally considered drugs, but they are covered by the Center for Biologics Evaluation and...
cautions that people with heart or lung disease need their supplementary oxygen carefully regulated and should not use oxygen bars.
Victorian society had a fascination for the rapidly expanding field of science. In "Dr. Ox's Experiment
Dr. Ox's Experiment
"Dr. Ox's Experiment" is a short story by the French writer and pioneer of science-fiction, Jules Verne, published in 1872. It describes an experiment by one Dr. Ox and his assistant Gedeon Ygene. A prosperous scientist Dr. Ox offers to build a novel gas lighting system to an unusually stuffy...
", a short story written by Jules Verne
Jules Verne
Jules Gabriel Verne was a French author who pioneered the science fiction genre. He is best known for his novels Twenty Thousand Leagues Under the Sea , A Journey to the Center of the Earth , and Around the World in Eighty Days...
in 1872, the eponymous doctor uses electrolysis of water
Electrolysis of water
Electrolysis of water is the decomposition of water into oxygen and hydrogen gas due to an electric current being passed through the water.-Principle:...
to separate oxygen and hydrogen. He then pumps the pure oxygen throughout the town of Quiquendone, causing the normally tranquil inhabitants and their animals to become aggressive and plants to grow rapidly. An explosion of the hydrogen and oxygen in Dr Ox's factory brings his experiment to an end. Verne summarised his story by explaining that the effects of oxygen described in the tale were his own invention. There is also a brief episode of oxygen intoxication in his "From the Earth to the Moon
From the Earth to the Moon
From the Earth to the Moon is a humorous science fantasy novel by Jules Verne and is one of the earliest entries in that genre. It tells the story of the president of a post-American Civil War gun club in Baltimore, his rival, a Philadelphia maker of armor, and a Frenchman, who build an enormous...
".
See also
- Effect of oxygen on chronic obstructive pulmonary diseaseEffect of oxygen on chronic obstructive pulmonary diseaseIn some individuals, the effect of oxygen on chronic obstructive pulmonary disease is to cause increased carbon dioxide retention, which may cause drowsiness, headaches, and in severe cases lack of respiration, which may lead to death...
- Nitrogen narcosisNitrogen narcosisNarcosis while diving , is a reversible alteration in consciousness that occurs while scuba diving at depth. The Greek word ναρκωσις is derived from narke, "temporary decline or loss of senses and movement, numbness", a term used by Homer and Hippocrates...
Sources
- Revised version of Donald's articles also available as:
External links
GeneralThe following external site is a compendium of resources:
- Rubicon Research Repository. – Online collection of the oxygen toxicity research
Specialised
The following external sites contain resources specific to particular topics:
- 2008 Divers Alert Network Technical Diving Conference. – Video of "Oxygen Toxicity" lecture by Dr. Richard Vann (free download, mp4, 86MB).. – Wide and detailed discussion of the effects of breathing oxygen on the respiratory system. – Concise clinical overview with extensive references.