
Osteosarcoma
Encyclopedia
Osteosarcoma is an aggressive cancerous neoplasm arising from primitive transformed cells of mesenchymal
origin that exhibit osteoblast
ic differentiation and produce malignant
osteoid
. It is the most common histological form of primary bone cancer.
Incidence rates for osteosarcoma in U.S. patients under 20 years of age are estimated at 5.0 per million per year in the general population, with a slight variation between individuals of black, Hispanic, and white ethnicities (6.8, 6.5, and 4.6 per million per year, respectively). It is slightly more common in males (5.4 per million per year) than in females (4.0 per million per year).
There is a preference for origination in the metaphyseal
region of tubular long bone
s, with 42% occurring in the femur, 19% in the tibia, and 10% in the humerus. About 8% of all cases occur in the skull and jaw, and another 8% in the pelvis.
in children under age 15. Osteogenic sarcoma affects 400 children under age 20 and 500 adults (most between the ages of 15-30) every year in the USA
. Approximately 1/3 of the 900 will die each year, or about 300 a year. A second peak in incidence occurs in the elderly, usually associated with an underlying bone pathology such as Paget's disease
, medullary infarct, or prior irradiation
.
2. Bone dysplasias, including Paget's disease, fibrous dysplasia, enchondromatosis, and hereditary multiple exostoses, increase the risk of osteosarcoma.
3. Li-Fraumeni syndrome (germline TP53 mutation) is a predisposing factor for osteosarcoma development.
4. Rothmund-Thomson syndrome (i.e. autosomal recessive association of congenital bone defects, hair and skin dysplasias, hypogonadism, cataracts) is associated with increased risk of osteosarcoma.
2. Multifocal
3. Telangiectatic
4. Small cell
5. Intraosseous well-differentiated
6. Intracortical
7. Periosteal
8. Paraosteal
9. High-grade surface
10. Extraosseous
Although about 90% of patients are able to have limb-salvage surgery, complications - particularly infection, prosthetic loosening and non-union - or local tumor recurrence may cause the need for further surgery or amputation.
Mifamurtide
is used after a patient has had surgery to remove the tumor and together with chemotherapy to kill remaining cancer cells to reduce the risk of cancer coming back.
 The tumor may be localized at the end of the long bone. Most often it affects the upper end of tibia
The tumor may be localized at the end of the long bone. Most often it affects the upper end of tibia
or humerus
, or lower end of femur
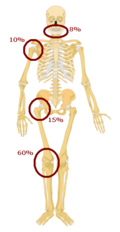
. Osteosarcoma tends to affect regions around the knee
in 60% of cases, 15% around the hip, 10% at the shoulder
, and 8% in the jaw
. The tumor is solid, hard, irregular ("fir-tree," "moth-eaten" or "sun-burst" appearance on X-ray examination) due to the tumor spicules of calcified bone radiating in right angles. These right angles form what is known as Codman's triangle. Surrounding tissues are infiltrated.
Microscopically: The characteristic feature of osteosarcoma is presence of osteoid (bone formation) within the tumor. Tumor cells are very pleomorphic
(anaplastic), some are giant, numerous atypical mitoses. These cells produce osteoid
describing irregular trabeculae (amorphous, eosinophilic
/pink) with or without central calcification (hematoxylinophilic/blue, granular) - tumor bone. Tumor cells are included in the osteoid
matrix. Depending on the features of the tumor cells present (whether they resemble bone cells, cartilage cells or fibroblast cells), the tumor can be subclassified. Osteosarcomas may exhibit multinucleated osteoclast-like giant cells.
Several research groups are investigating cancer stem cells and their potential to cause tumors. The connection between osteosarcoma and fluoride has been investigated; there is some association between water fluoridation
and deaths due to osteosarcoma. One study showed 6.9 times the occurrence of osteosarcoma in fluoridated communities compared to non-fluoridated areas. Radiotherapy for unrelated conditions may be a rare cause.
bone tumor (most bone tumors are benign
). Thus, many patients are initially misdiagnosed with cysts or muscle problems, and some are sent straight to physical therapy
without an x-ray
.
The route to osteosarcoma diagnosis usually begins with an x-ray
, continues with a combination of scans (CT scan, PET scan, bone scan, MRI) and ends with a surgical biopsy
. A characteristic often seen in an X-ray is the 'Codman's Triangle' which is basically a subperiosteal lesion formed when the periosteum is raised due to the tumor.
Films are suggestive, but bone biopsy
is the only definitive method to determine whether a tumor is malignant
or benign
.
The biopsy of suspected osteosarcoma should be performed by a qualified orthopedic oncologist
. The American Cancer Society
states: "Probably in no other cancer
is it as important to perform this procedure properly. An improperly performed biopsy
may make it difficult to save the affected limb from amputation
."
experienced in managing sarcomas. Current standard treatment is to use neoadjuvant chemotherapy
(chemotherapy
given before surgery
) followed by surgical resection. The percentage of tumor cell necrosis
(cell death) seen in the tumor after surgery gives an idea of the prognosis and also lets the oncologist know if the chemotherapy
regime should be altered after surgery.
Standard therapy is a combination of limb-salvage orthopedic surgery
when possible (or amputation in some cases) and a combination of high dose methotrexate
with leucovorin rescue, intra-arterial cisplatin
, adriamycin, ifosfamide
with mesna
, BCD
, etoposide
, muramyl tri-peptite (MTP). Rotationplasty is also another surgical technique that may be used. Ifosfamide can be used as an adjuvant treatment if the necrosis
rate is low.
Despite the success of chemotherapy for osteosarcoma, it has one of the lowest survival rates for pediatric cancer. The best reported 10-year survival rate is 92%; the protocol used is an aggressive intra-arterial regimen that individualizes therapy based on arteriographic response. Three-year event-free survival ranges from 50% to 75%, and five-year survival ranges from 60% to 85+% in some studies. Overall, 65-70% patients treated five years ago will be alive today . These survival rates are overall averages and vary greatly depending on the individual necrosis rate.
Fluids are given for hydration, while drugs like Kytril and Zofran help with nausea
and vomiting
. Neupogen and Neulasta help with white blood cell
counts and neutrophil counts. Blood transfusions and epogen help with anemia
.
funds research and provides information on Ewing sarcoma and other bone cancers. This includes information for teenagers who have this condition.

s, Greyhound
s, German Shepherd
s, Rottweiler
s, mountain breeds (great Pyrenees, St. Bernard, Leonberger, Newfoundland), Doberman Pinschers and Great Dane
s. It has a ten times greater incidence
in dogs than humans. A hereditary
base has been shown in St. Bernard dogs. Spayed/neutered
dogs have twice the risk of intact ones to develop osteosarcoma. Infestation with the parasite Spirocerca lupi
can cause osteosarcoma of the esophagus
.
, the distal radius
, the distal femur
, and the tibia
, following the basic premise "far from the elbow, close to the knee". Other sites include the ribs, the mandible, the spine, and the pelvis. Rarely, osteosarcoma may arise from soft-tissues (extraskeletal osteosarcoma). Metastasis
of tumors involving the limb bones is very common, usually to the lungs. The tumor causes a great deal of pain, and can even lead to fracture of the affected bone. As with human osteosarcoma, bone biopsy
is the definitive method to reach a final diagnosis. Osteosarcoma should be differentiated from other bone tumours and a range of other lesions, such as osteomyelitis
. Differential diagnosis of the osteosarcoma of the skull in particular includes, among others, chondrosarcoma
and the multilobular tumour of bone
.
combined with amputation improves the survival time, but most dogs still die within a year. There are surgical techniques designed to save the leg (limb-sparing procedures), but they do not improve the prognosis. One key difference between osteosarcoma in dogs and humans is that the cancer is far more likely to spread to the lungs in dogs.
Some current studies indicate that osteoclast
inhibitors such as alendronate and pamidronate may have beneficial effects on the quality of life by reducing osteolysis, thus reducing the degree of pain as well as the risk of pathological fractures.
(apSTAR Veterinary Cancer Laser System: The use of a laser combined with a polymer has been shown to enhance tumor immunity and improve the rate of primary and metastatic tumor regression in laboratory models of tumors. IMULAN BioTherapeutics, LLC
has recently started examining the use of this laser device, termed apSTAR, for dogs with osteosarcoma and other tumor types.

Mesenchyme
Mesenchyme, or mesenchymal connective tissue, is a type of undifferentiated loose connective tissue that is derived mostly from mesoderm, although some are derived from other germ layers; e.g. some mesenchyme is derived from neural crest cells and thus originates from the ectoderm...
origin that exhibit osteoblast
Osteoblast
Osteoblasts are mononucleate cells that are responsible for bone formation; in essence, osteoblasts are specialized fibroblasts that in addition to fibroblastic products, express bone sialoprotein and osteocalcin.Osteoblasts produce a matrix of osteoid, which is composed mainly of Type I collagen...
ic differentiation and produce malignant
Malignant
Malignancy is the tendency of a medical condition, especially tumors, to become progressively worse and to potentially result in death. Malignancy in cancers is characterized by anaplasia, invasiveness, and metastasis...
osteoid
Osteoid
In histology, osteoid is the unmineralized, organic portion of the bone matrix that forms prior to the maturation of bone tissue. Osteoblasts begin the process of forming bone tissue by secreting the osteoid as several specific proteins...
. It is the most common histological form of primary bone cancer.
Incidence
Osteosarcoma is the eighth most common form of childhood cancer, comprising 2.4% of all malignancies in pediatric patients, and approximately 20% of all primary bone cancers.Incidence rates for osteosarcoma in U.S. patients under 20 years of age are estimated at 5.0 per million per year in the general population, with a slight variation between individuals of black, Hispanic, and white ethnicities (6.8, 6.5, and 4.6 per million per year, respectively). It is slightly more common in males (5.4 per million per year) than in females (4.0 per million per year).
There is a preference for origination in the metaphyseal
Metaphysis
The metaphysis is the wider portion of a long bone adjacent to the epiphyseal plate. It is this part of the bone that grows during childhood; as it grows, it ossifies near the diaphysis and the epiphyses...
region of tubular long bone
Bone
Bones are rigid organs that constitute part of the endoskeleton of vertebrates. They support, and protect the various organs of the body, produce red and white blood cells and store minerals. Bone tissue is a type of dense connective tissue...
s, with 42% occurring in the femur, 19% in the tibia, and 10% in the humerus. About 8% of all cases occur in the skull and jaw, and another 8% in the pelvis.
Prevalence
Osteogenic sarcoma is the sixth leading cancerCancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
in children under age 15. Osteogenic sarcoma affects 400 children under age 20 and 500 adults (most between the ages of 15-30) every year in the USA
United States
The United States of America is a federal constitutional republic comprising fifty states and a federal district...
. Approximately 1/3 of the 900 will die each year, or about 300 a year. A second peak in incidence occurs in the elderly, usually associated with an underlying bone pathology such as Paget's disease
Paget's disease of bone
Paget's disease is a chronic disorder that can result in enlarged and misshapen bones. The excessive breakdown and formation of bone tissue causes affected bone to weaken, resulting in pain, misshapen bones, fractures, and arthritis in the joints near the affected bones...
, medullary infarct, or prior irradiation
Irradiation
Irradiation is the process by which an object is exposed to radiation. The exposure can originate from various sources, including natural sources. Most frequently the term refers to ionizing radiation, and to a level of radiation that will serve a specific purpose, rather than radiation exposure to...
.
Genetic Predisposition
1. Familial cases where the deletion of chromosome 13q14 thus inactivating the retinoblastoma gene (RB gene) and is associated with high risk of osteosarcoma to develop.2. Bone dysplasias, including Paget's disease, fibrous dysplasia, enchondromatosis, and hereditary multiple exostoses, increase the risk of osteosarcoma.
3. Li-Fraumeni syndrome (germline TP53 mutation) is a predisposing factor for osteosarcoma development.
4. Rothmund-Thomson syndrome (i.e. autosomal recessive association of congenital bone defects, hair and skin dysplasias, hypogonadism, cataracts) is associated with increased risk of osteosarcoma.
Variants
1. Conventional: Osteoblastic, Chondroblastic, Fibroblastic2. Multifocal
3. Telangiectatic
4. Small cell
5. Intraosseous well-differentiated
6. Intracortical
7. Periosteal
8. Paraosteal
9. High-grade surface
10. Extraosseous
Treatment
Complete radical surgical en bloc resection is the treatment of choice in osteosarcoma.Although about 90% of patients are able to have limb-salvage surgery, complications - particularly infection, prosthetic loosening and non-union - or local tumor recurrence may cause the need for further surgery or amputation.
Mifamurtide
Mifamurtide
Mifamurtide is a drug against osteosarcoma, a kind of bone cancer mainly affecting children and young adults, which is lethal in about a third of cases. The drug was approved in Europe in March 2009.- History :...
is used after a patient has had surgery to remove the tumor and together with chemotherapy to kill remaining cancer cells to reduce the risk of cancer coming back.
Mortality and survival
Deaths due to malignant neoplasms of the bones and joints account for an unknown amount of childhood cancer deaths. Mortality rates due to osteosarcoma have been declining at approximately 1.3% per year. Long-term survival probabilities for osteosarcoma have improved dramatically during the late 20th century and approximated 68% in 2009.Pathology
Tibia
The tibia , shinbone, or shankbone is the larger and stronger of the two bones in the leg below the knee in vertebrates , and connects the knee with the ankle bones....
or humerus
Humerus
The humerus is a long bone in the arm or forelimb that runs from the shoulder to the elbow....
, or lower end of femur
Femur
The femur , or thigh bone, is the most proximal bone of the leg in tetrapod vertebrates capable of walking or jumping, such as most land mammals, birds, many reptiles such as lizards, and amphibians such as frogs. In vertebrates with four legs such as dogs and horses, the femur is found only in...
. Osteosarcoma tends to affect regions around the knee
Knee
The knee joint joins the thigh with the leg and consists of two articulations: one between the fibula and tibia, and one between the femur and patella. It is the largest joint in the human body and is very complicated. The knee is a mobile trocho-ginglymus , which permits flexion and extension as...
in 60% of cases, 15% around the hip, 10% at the shoulder
Shoulder
The human shoulder is made up of three bones: the clavicle , the scapula , and the humerus as well as associated muscles, ligaments and tendons. The articulations between the bones of the shoulder make up the shoulder joints. The major joint of the shoulder is the glenohumeral joint, which...
, and 8% in the jaw
Jaw
The jaw is any opposable articulated structure at the entrance of the mouth, typically used for grasping and manipulating food. The term jaws is also broadly applied to the whole of the structures constituting the vault of the mouth and serving to open and close it and is part of the body plan of...
. The tumor is solid, hard, irregular ("fir-tree," "moth-eaten" or "sun-burst" appearance on X-ray examination) due to the tumor spicules of calcified bone radiating in right angles. These right angles form what is known as Codman's triangle. Surrounding tissues are infiltrated.
Microscopically: The characteristic feature of osteosarcoma is presence of osteoid (bone formation) within the tumor. Tumor cells are very pleomorphic
Pleomorphism (cytology)
Pleomorphism is a term used in histology and cytopathology to describe variability in the size and shape of cells and/or their nuclei. It is a feature characteristic of malignant neoplasms....
(anaplastic), some are giant, numerous atypical mitoses. These cells produce osteoid
Osteoid
In histology, osteoid is the unmineralized, organic portion of the bone matrix that forms prior to the maturation of bone tissue. Osteoblasts begin the process of forming bone tissue by secreting the osteoid as several specific proteins...
describing irregular trabeculae (amorphous, eosinophilic
Eosinophilic
Eosinophilic refers to the staining of certain tissues, cells, or organelles after they have been washed with eosin, a dye.Eosin is an acidic dye; thus, the structure being stained is basic....
/pink) with or without central calcification (hematoxylinophilic/blue, granular) - tumor bone. Tumor cells are included in the osteoid
Osteoid
In histology, osteoid is the unmineralized, organic portion of the bone matrix that forms prior to the maturation of bone tissue. Osteoblasts begin the process of forming bone tissue by secreting the osteoid as several specific proteins...
matrix. Depending on the features of the tumor cells present (whether they resemble bone cells, cartilage cells or fibroblast cells), the tumor can be subclassified. Osteosarcomas may exhibit multinucleated osteoclast-like giant cells.
Causes
The causes of osteosarcoma are not known.Several research groups are investigating cancer stem cells and their potential to cause tumors. The connection between osteosarcoma and fluoride has been investigated; there is some association between water fluoridation
Water fluoridation
Water fluoridation is the controlled addition of fluoride to a public water supply to reduce tooth decay. Fluoridated water has fluoride at a level that is effective for preventing cavities; this can occur naturally or by adding fluoride...
and deaths due to osteosarcoma. One study showed 6.9 times the occurrence of osteosarcoma in fluoridated communities compared to non-fluoridated areas. Radiotherapy for unrelated conditions may be a rare cause.
Symptoms
Many patients first complain of pain that may be worse at night, and may have been occurring for some time. If the tumor is large, it can appear as a swelling. The affected bone is not as strong as normal bones and may fracture with minor trauma (a pathological fracture).Diagnosis
Family physicians and orthopedists rarely see a malignantMalignant
Malignancy is the tendency of a medical condition, especially tumors, to become progressively worse and to potentially result in death. Malignancy in cancers is characterized by anaplasia, invasiveness, and metastasis...
bone tumor (most bone tumors are benign
Benign
A benign tumor is a tumor that lacks the ability to metastasize. Common examples of benign tumors include moles and uterine fibroids.The term "benign" implies a mild and nonprogressive disease. Indeed, many kinds of benign tumors are harmless to human health...
). Thus, many patients are initially misdiagnosed with cysts or muscle problems, and some are sent straight to physical therapy
Physical therapy
Physical therapy , often abbreviated PT, is a health care profession. Physical therapy is concerned with identifying and maximizing quality of life and movement potential within the spheres of promotion, prevention, diagnosis, treatment/intervention,and rehabilitation...
without an x-ray
X-ray
X-radiation is a form of electromagnetic radiation. X-rays have a wavelength in the range of 0.01 to 10 nanometers, corresponding to frequencies in the range 30 petahertz to 30 exahertz and energies in the range 120 eV to 120 keV. They are shorter in wavelength than UV rays and longer than gamma...
.
The route to osteosarcoma diagnosis usually begins with an x-ray
X-ray
X-radiation is a form of electromagnetic radiation. X-rays have a wavelength in the range of 0.01 to 10 nanometers, corresponding to frequencies in the range 30 petahertz to 30 exahertz and energies in the range 120 eV to 120 keV. They are shorter in wavelength than UV rays and longer than gamma...
, continues with a combination of scans (CT scan, PET scan, bone scan, MRI) and ends with a surgical biopsy
Biopsy
A biopsy is a medical test involving sampling of cells or tissues for examination. It is the medical removal of tissue from a living subject to determine the presence or extent of a disease. The tissue is generally examined under a microscope by a pathologist, and can also be analyzed chemically...
. A characteristic often seen in an X-ray is the 'Codman's Triangle' which is basically a subperiosteal lesion formed when the periosteum is raised due to the tumor.
Films are suggestive, but bone biopsy
Biopsy
A biopsy is a medical test involving sampling of cells or tissues for examination. It is the medical removal of tissue from a living subject to determine the presence or extent of a disease. The tissue is generally examined under a microscope by a pathologist, and can also be analyzed chemically...
is the only definitive method to determine whether a tumor is malignant
Malignant
Malignancy is the tendency of a medical condition, especially tumors, to become progressively worse and to potentially result in death. Malignancy in cancers is characterized by anaplasia, invasiveness, and metastasis...
or benign
Benign
A benign tumor is a tumor that lacks the ability to metastasize. Common examples of benign tumors include moles and uterine fibroids.The term "benign" implies a mild and nonprogressive disease. Indeed, many kinds of benign tumors are harmless to human health...
.
The biopsy of suspected osteosarcoma should be performed by a qualified orthopedic oncologist
Orthopedic oncologist
An orthopedic oncologist is a medical doctor and surgeon who specializes in the diagnoses and treatment of primary benign and malignant tumors of the bones. An orthopedic oncologist in the United States must complete 4 years of medical school. Following graduation from medical school, the...
. The American Cancer Society
American Cancer Society
The American Cancer Society is the "nationwide community-based voluntary health organization" dedicated, in their own words, "to eliminating cancer as a major health problem by preventing cancer, saving lives, and diminishing suffering from cancer, through research, education, advocacy, and...
states: "Probably in no other cancer
Cancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
is it as important to perform this procedure properly. An improperly performed biopsy
Biopsy
A biopsy is a medical test involving sampling of cells or tissues for examination. It is the medical removal of tissue from a living subject to determine the presence or extent of a disease. The tissue is generally examined under a microscope by a pathologist, and can also be analyzed chemically...
may make it difficult to save the affected limb from amputation
Amputation
Amputation is the removal of a body extremity by trauma, prolonged constriction, or surgery. As a surgical measure, it is used to control pain or a disease process in the affected limb, such as malignancy or gangrene. In some cases, it is carried out on individuals as a preventative surgery for...
."
Treatment
Patients with osteosarcoma are best managed by a medical oncologist and an orthopedic oncologistOrthopedic oncologist
An orthopedic oncologist is a medical doctor and surgeon who specializes in the diagnoses and treatment of primary benign and malignant tumors of the bones. An orthopedic oncologist in the United States must complete 4 years of medical school. Following graduation from medical school, the...
experienced in managing sarcomas. Current standard treatment is to use neoadjuvant chemotherapy
Chemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
(chemotherapy
Chemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
given before surgery
Surgery
Surgery is an ancient medical specialty that uses operative manual and instrumental techniques on a patient to investigate and/or treat a pathological condition such as disease or injury, or to help improve bodily function or appearance.An act of performing surgery may be called a surgical...
) followed by surgical resection. The percentage of tumor cell necrosis
Necrosis
Necrosis is the premature death of cells in living tissue. Necrosis is caused by factors external to the cell or tissue, such as infection, toxins, or trauma. This is in contrast to apoptosis, which is a naturally occurring cause of cellular death...
(cell death) seen in the tumor after surgery gives an idea of the prognosis and also lets the oncologist know if the chemotherapy
Chemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
regime should be altered after surgery.
Standard therapy is a combination of limb-salvage orthopedic surgery
Orthopedic surgery
Orthopedic surgery or orthopedics is the branch of surgery concerned with conditions involving the musculoskeletal system...
when possible (or amputation in some cases) and a combination of high dose methotrexate
Methotrexate
Methotrexate , abbreviated MTX and formerly known as amethopterin, is an antimetabolite and antifolate drug. It is used in treatment of cancer, autoimmune diseases, ectopic pregnancy, and for the induction of medical abortions. It acts by inhibiting the metabolism of folic acid. Methotrexate...
with leucovorin rescue, intra-arterial cisplatin
Cisplatin
Cisplatin, cisplatinum, or cis-diamminedichloroplatinum is a chemotherapy drug. It is used to treat various types of cancers, including sarcomas, some carcinomas , lymphomas, and germ cell tumors...
, adriamycin, ifosfamide
Ifosfamide
Ifosfamide is a nitrogen mustard alkylating agent used in the treatment of cancer.It is sometimes abbreviated "IFO".-Uses:It is given as a treatment for a variety of cancers, including:...
with mesna
Mesna
Mesna is an organosulfur compound. It is used in cancer chemotherapy involving cyclophosphamide and ifosfamide as an adjuvant. It is marketed by Baxter as Uromitexan and Mesnex...
, BCD
BCD
BCD may refer to:* Binary coded decimal, representation of individual decimal digits in binary.* Bad Conduct Discharge, a form of discharge from US military service* Barrels per calendar day, a unit for measuring output of oil refineries...
, etoposide
Etoposide
Etoposide phosphate is an anti-cancer agent. It is known in the laboratory as a topoisomerase poison. Etoposide is often incorrectly referred to as a topoisomerase inhibitor in order to avoid using the term "poison" in a clinical setting...
, muramyl tri-peptite (MTP). Rotationplasty is also another surgical technique that may be used. Ifosfamide can be used as an adjuvant treatment if the necrosis
Necrosis
Necrosis is the premature death of cells in living tissue. Necrosis is caused by factors external to the cell or tissue, such as infection, toxins, or trauma. This is in contrast to apoptosis, which is a naturally occurring cause of cellular death...
rate is low.
Despite the success of chemotherapy for osteosarcoma, it has one of the lowest survival rates for pediatric cancer. The best reported 10-year survival rate is 92%; the protocol used is an aggressive intra-arterial regimen that individualizes therapy based on arteriographic response. Three-year event-free survival ranges from 50% to 75%, and five-year survival ranges from 60% to 85+% in some studies. Overall, 65-70% patients treated five years ago will be alive today . These survival rates are overall averages and vary greatly depending on the individual necrosis rate.
Fluids are given for hydration, while drugs like Kytril and Zofran help with nausea
Nausea
Nausea , is a sensation of unease and discomfort in the upper stomach with an involuntary urge to vomit. It often, but not always, precedes vomiting...
and vomiting
Vomiting
Vomiting is the forceful expulsion of the contents of one's stomach through the mouth and sometimes the nose...
. Neupogen and Neulasta help with white blood cell
White blood cell
White blood cells, or leukocytes , are cells of the immune system involved in defending the body against both infectious disease and foreign materials. Five different and diverse types of leukocytes exist, but they are all produced and derived from a multipotent cell in the bone marrow known as a...
counts and neutrophil counts. Blood transfusions and epogen help with anemia
Anemia
Anemia is a decrease in number of red blood cells or less than the normal quantity of hemoglobin in the blood. However, it can include decreased oxygen-binding ability of each hemoglobin molecule due to deformity or lack in numerical development as in some other types of hemoglobin...
.
Prognosis
Prognosis is separated into three groups.- Stage I osteosarcoma is rare and includes parosteal osteosarcoma or low-grade central osteosarcoma. It has an excellent prognosis (>90%) with wide resection.
- Stage II prognosis depends on the site of the tumor (proximal tibia, femur, pelvis, etc.), size of the tumor mass (in cm.), and the degree of necrosis from neoadjuvant chemotherapy (chemotherapy prior to surgery). Other pathological factors such as the degree of p-glycoprotein, whether the tumor is cxcr4-positive, or Her2-positive are also important, as these are associated with distant metastases to the lung. The prognosis for patients with metastatic osteosarcoma improves with longer times to metastases, (more than 12 months-24 months), a smaller number of metastases, and their resectability. It is better to have fewer metastases than longer time to metastases. Those with a longer length of time(>24months) and few nodules (two or fewer) have the best prognosis with a 2-year survival after the metastases of 50%, 5-year of 40% and 10 year of 20%. If metastases are both local and regional, the prognosis is worse.
- Initial presentation of stage III osteosarcoma with lung metastases depends on the resectability of the primary tumor and lung noduleNodule (medicine)For use of the term nodule in dermatology, see Nodule In medicine, a nodule refers to a relatively hard, roughly spherical abnormal structure....
s, degree of necrosis of the primary tumor, and maybe the number of metastases. Overall survival prognosis is about 30%.
Research, information and support
In the UK and Ireland The Bone Cancer Research Trust (BCRT)The Bone Cancer Research Trust (BCRT)
The Bone Cancer Research Trust is a charity providing funding for research into primary bone cancer, raising awareness of the disease, providing patient information and support services...
funds research and provides information on Ewing sarcoma and other bone cancers. This includes information for teenagers who have this condition.
Canine osteosarcoma
Risk factors
Osteosarcoma is the most common bone tumor in dogs and typically afflicts middle-age large and giant breed dogs such as Irish WolfhoundIrish Wolfhound
The Irish wolfhound is a breed of domestic dog , specifically a sighthound. The name originates from its purpose rather than from its appearance...
s, Greyhound
Greyhound
The Greyhound is a breed of sighthound that has been primarily bred for coursing game and racing, and the breed has also recently seen a resurgence in its popularity as a pedigree show dog and family pet. It is a gentle and intelligent breed...
s, German Shepherd
German Shepherd Dog
The German Shepherd Dog , also known as an Alsatian or just the German Shepherd, is a breed of large-sized dog that originated in Germany. The German Shepherd is a relatively new breed of dog, with its origin dating to 1899. As part of the Herding Group, the German Shepherd is a working dog...
s, Rottweiler
Rottweiler
The Rottweiler is a medium to large size breed of domestic dog that originated in Rottweil, Germany. The dogs were known as "Rottweil butchers' dogs" because they were used to herd livestock and pull carts laden with butchered meat and other products to market...
s, mountain breeds (great Pyrenees, St. Bernard, Leonberger, Newfoundland), Doberman Pinschers and Great Dane
Great Dane
The Great Dane , also known as German Mastiff or Danish Hound , is a breed of domestic dog known for its giant size...
s. It has a ten times greater incidence
Incidence (epidemiology)
Incidence is a measure of the risk of developing some new condition within a specified period of time. Although sometimes loosely expressed simply as the number of new cases during some time period, it is better expressed as a proportion or a rate with a denominator.Incidence proportion is the...
in dogs than humans. A hereditary
Heredity
Heredity is the passing of traits to offspring . This is the process by which an offspring cell or organism acquires or becomes predisposed to the characteristics of its parent cell or organism. Through heredity, variations exhibited by individuals can accumulate and cause some species to evolve...
base has been shown in St. Bernard dogs. Spayed/neutered
Neutering
Neutering, from the Latin neuter , is the removal of an animal's reproductive organ, either all of it or a considerably large part. The process is often used in reference to males whereas spaying is often reserved for females. Colloquially, both terms are often referred to as fixing...
dogs have twice the risk of intact ones to develop osteosarcoma. Infestation with the parasite Spirocerca lupi
Spirocerca lupi
Spirocerca lupi is a species of nematode. In dogs, infestation can cause osteosarcoma of the esophagus. Doramectin has been used against it....
can cause osteosarcoma of the esophagus
Esophagus
The esophagus is an organ in vertebrates which consists of a muscular tube through which food passes from the pharynx to the stomach. During swallowing, food passes from the mouth through the pharynx into the esophagus and travels via peristalsis to the stomach...
.
Clinical presentation
The most commonly affected bones are the proximal humerusHumerus
The humerus is a long bone in the arm or forelimb that runs from the shoulder to the elbow....
, the distal radius
Radius (bone)
The radius is one of the two large bones of the forearm, the other being the ulna. It extends from the lateral side of the elbow to the thumb side of the wrist and runs parallel to the ulna, which exceeds it in length and size. It is a long bone, prism-shaped and slightly curved longitudinally...
, the distal femur
Femur
The femur , or thigh bone, is the most proximal bone of the leg in tetrapod vertebrates capable of walking or jumping, such as most land mammals, birds, many reptiles such as lizards, and amphibians such as frogs. In vertebrates with four legs such as dogs and horses, the femur is found only in...
, and the tibia
Tibia
The tibia , shinbone, or shankbone is the larger and stronger of the two bones in the leg below the knee in vertebrates , and connects the knee with the ankle bones....
, following the basic premise "far from the elbow, close to the knee". Other sites include the ribs, the mandible, the spine, and the pelvis. Rarely, osteosarcoma may arise from soft-tissues (extraskeletal osteosarcoma). Metastasis
Metastasis
Metastasis, or metastatic disease , is the spread of a disease from one organ or part to another non-adjacent organ or part. It was previously thought that only malignant tumor cells and infections have the capacity to metastasize; however, this is being reconsidered due to new research...
of tumors involving the limb bones is very common, usually to the lungs. The tumor causes a great deal of pain, and can even lead to fracture of the affected bone. As with human osteosarcoma, bone biopsy
Biopsy
A biopsy is a medical test involving sampling of cells or tissues for examination. It is the medical removal of tissue from a living subject to determine the presence or extent of a disease. The tissue is generally examined under a microscope by a pathologist, and can also be analyzed chemically...
is the definitive method to reach a final diagnosis. Osteosarcoma should be differentiated from other bone tumours and a range of other lesions, such as osteomyelitis
Osteomyelitis
Osteomyelitis simply means an infection of the bone or bone marrow...
. Differential diagnosis of the osteosarcoma of the skull in particular includes, among others, chondrosarcoma
Chondrosarcoma
Chondrosarcoma is a cancer composed of cells derived from transformed cells that produce cartilage. Chondrosarcoma is a member of a category of "soft tissue" malignancies known as sarcomas. About 30% of skeletal system cancers are chondrosarcomas...
and the multilobular tumour of bone
Multilobular tumour of bone
The Multilobular tumour of bone , although uncommon, is the most common tumour of the canine skull.MTB usually presents as a firm, circumscribed and generally slowgrowing bone tumour in older dogs from medium or large breeds. Its biological behaviour may range from benign to malignant, as it has...
.
Treatment and prognosis
Amputation of the leg is the initial treatment, although this alone will not prevent metastasis. ChemotherapyChemotherapy
Chemotherapy is the treatment of cancer with an antineoplastic drug or with a combination of such drugs into a standardized treatment regimen....
combined with amputation improves the survival time, but most dogs still die within a year. There are surgical techniques designed to save the leg (limb-sparing procedures), but they do not improve the prognosis. One key difference between osteosarcoma in dogs and humans is that the cancer is far more likely to spread to the lungs in dogs.
Some current studies indicate that osteoclast
Osteoclast
An osteoclast is a type of bone cell that removes bone tissue by removing its mineralized matrix and breaking up the organic bone . This process is known as bone resorption. Osteoclasts were discovered by Kolliker in 1873...
inhibitors such as alendronate and pamidronate may have beneficial effects on the quality of life by reducing osteolysis, thus reducing the degree of pain as well as the risk of pathological fractures.
Experimental laser procedure
Autologous patient specific tumor antigen responseAutologous patient specific tumor antigen response
Autologous Patient Specific Tumor Antigen Response technology, or apSTAR, is a new cancer treatment procedure being developed by IMULAN BioTherapeutics, LLC and for comparative oncology....
(apSTAR Veterinary Cancer Laser System: The use of a laser combined with a polymer has been shown to enhance tumor immunity and improve the rate of primary and metastatic tumor regression in laboratory models of tumors. IMULAN BioTherapeutics, LLC
IMULAN BioTherapeutics, LLC
-About:IMULAN BioTherapeutics, LLC, is a veterinary immunobiology company developing a range of immune based therapies for veterinary medicine. IMULAN BioTherapeutics, LLC has several divisions related to immuno-biology and comparative medicine....
has recently started examining the use of this laser device, termed apSTAR, for dogs with osteosarcoma and other tumor types.
Osteosarcoma in cats
Osteosarcoma is also the most common bone tumor in the cat, although not as frequently encountered, and most typically affects the rear legs. The cancer is less aggressive in cats than in dogs, and therefore amputation alone can lead to a significant survival time.People diagnosed with osteosarcoma
- Antonietta MeoAntonietta MeoThe Venerable Antonietta Meo was an Italian girl who may become the youngest saint ever canonized by the Roman Catholic Church.-Life and death:...
- Terry FoxTerry FoxTerrance Stanley "Terry" Fox , was a Canadian humanitarian, athlete, and cancer research activist. In 1980, with one leg having been amputated, he embarked on a cross-Canada run to raise money and awareness for cancer research...
- Edward M. Kennedy, Jr.
- Bruce FeilerBruce FeilerBruce Feiler is a popular American writer on faith, family, and finding meaning in everyday life. He is the best-selling author of nine books, including Walking the Bible, Abraham, and America's Prophet, and one of only a handful of writers to have four consecutive New York Times nonfiction...
- Wayman TisdaleWayman TisdaleWayman Lawrence Tisdale was an American professional basketball player in the NBA and a smooth jazz bass guitarist. A three-time All American at the University of Oklahoma, he was elected to the National Collegiate Basketball Hall of Fame in 2009.-Early life:Tisdale was born in Fort Worth, Texas...