
Nitrogen narcosis
Overview
Narcosis while diving (also known as nitrogen narcosis, inert gas narcosis, raptures of the deep, Martini effect), is a reversible alteration in consciousness
Consciousness
Consciousness is a term that refers to the relationship between the mind and the world with which it interacts. It has been defined as: subjectivity, awareness, the ability to experience or to feel, wakefulness, having a sense of selfhood, and the executive control system of the mind...
that occurs while scuba diving
Scuba diving
Scuba diving is a form of underwater diving in which a diver uses a scuba set to breathe underwater....
at depth. The Greek word ναρκωσις (narcosis) is derived from narke, "temporary decline or loss of senses and movement, numbness", a term used by Homer
Homer
In the Western classical tradition Homer , is the author of the Iliad and the Odyssey, and is revered as the greatest ancient Greek epic poet. These epics lie at the beginning of the Western canon of literature, and have had an enormous influence on the history of literature.When he lived is...
and Hippocrates
Hippocrates
Hippocrates of Cos or Hippokrates of Kos was an ancient Greek physician of the Age of Pericles , and is considered one of the most outstanding figures in the history of medicine...
. Narcosis produces a state similar to alcohol intoxication
Drunkenness
Alcohol intoxication is a physiological state that occurs when a person has a high level of ethanol in his or her blood....
or nitrous oxide
Nitrous oxide
Nitrous oxide, commonly known as laughing gas or sweet air, is a chemical compound with the formula . It is an oxide of nitrogen. At room temperature, it is a colorless non-flammable gas, with a slightly sweet odor and taste. It is used in surgery and dentistry for its anesthetic and analgesic...
inhalation, and can occur during shallow dives, but usually does not become noticeable until greater depths, beyond 30 metres (98.4 ft).
Apart from helium
Helium
Helium is the chemical element with atomic number 2 and an atomic weight of 4.002602, which is represented by the symbol He. It is a colorless, odorless, tasteless, non-toxic, inert, monatomic gas that heads the noble gas group in the periodic table...
, and probably neon
Neon
Neon is the chemical element that has the symbol Ne and an atomic number of 10. Although a very common element in the universe, it is rare on Earth. A colorless, inert noble gas under standard conditions, neon gives a distinct reddish-orange glow when used in either low-voltage neon glow lamps or...
, all gases that can be breathed
Breathing gas
Breathing gas is a mixture of gaseous chemical elements and compounds used for respiration.Air is the most common and only natural breathing gas...
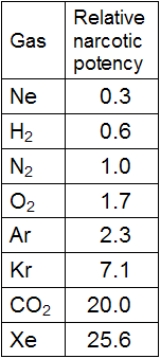
have a narcotic effect, which is greater as the lipid solubility of the gas increases.