

Gastritis
Encyclopedia
Gastritis is an inflammation of the lining of the stomach, and has many possible causes. The main acute causes are excessive alcohol
consumption or prolonged use of nonsteroidal anti-inflammatory drugs (also known as NSAIDs) such as aspirin
or ibuprofen
. Sometimes gastritis develops after major surgery, traumatic injury, burns, or severe infections. Gastritis may also occur in those who have had weight loss surgery resulting in the banding
or reconstruction of the digestive tract. Chronic causes are infection with bacteria, primarily Helicobacter pylori
, chronic bile reflux
, stress and certain autoimmune disorders can cause gastritis as well. The most common symptom is abdominal upset or pain. Other symptoms are indigestion, abdominal bloating, nausea, and vomiting and pernicious anemia
. Some may have a feeling of fullness or burning in the upper abdomen. A gastroscopy, blood test, complete blood count test, or a stool test may be used to diagnose gastritis. Treatment includes taking antacids or other medicines, such as proton pump inhibitors or antibiotics, and avoiding hot or spicy foods. For those with pernicious anemia
, B12 injections are given.
 Many people with gastritis experience no symptoms at all. However, upper central abdominal pain
Many people with gastritis experience no symptoms at all. However, upper central abdominal pain
is the most common symptom; the pain may be dull, vague, burning, aching, gnawing, sore, or sharp. Pain is usually located in the upper central portion of the abdomen, but it may occur anywhere from the upper left portion of the abdomen around to the back.
Other signs and symptoms may include:
secretion. High doses of alcohol do not stimulate secretion of acid. NSAIDs inhibit cyclooxygenase-1, or COX-1, an enzyme responsible for the biosynthesis of eicosanoids in the stomach, which increases the possibility of peptic ulcers forming. Also, NSAIDs, such as aspirin, reduce a substance that protects the stomach called prostaglandin
. These drugs used in a short period are not typically dangerous. However, regular use can lead to gastritis.
, certain connective tissue disorders, and liver or kidney failure.
, the reversible replacement of differentiated cells, occurs in the setting of severe damage of the gastric glands, which then waste away (atrophic gastritis
), which are progressively replaced by mucous glands. Gastric ulcers may develop; it is unclear if they are the causes or the consequences. Intestinal metaplasia typically begins in response to chronic mucosal injury in the antrum
, and may extend to the body. Gastric mucosa cells change to resemble intestinal mucosa and may even assume absorptive characteristics. Intestinal metaplasia
is classified histologically as complete or incomplete. With complete metaplasia, gastric mucosa is completely transformed into small-bowel mucosa, both histologically and functionally, with the ability to absorb nutrients and secrete peptides. In incomplete metaplasia, the epithelium assumes a histologic appearance closer to that of the large intestine and frequently exhibits dysplasia.
colonizes the stomach of more than half of the world's population, and the infection continues to play a key role in the pathogenesis of a number of gastroduodenal diseases. Colonization of the gastric mucosa with Helicobacter pylori results in the development of chronic gastritis in infected individuals and in a subset of patients chronic gastritis progresses to complications (i.e. ulcer disease, gastric neoplasias, some distinct extra gastric disorders). However, gastritis has no adverse consequences for most hosts and emerging evidence suggests that H. pylori prevalence is inversely related to gastroesophageal reflux disease
and allergic disorders. These observations indicate that eradication may not be appropriate for certain populations due to the potentially beneficial effects conferred by persistent gastric inflammation.
relief. When antacids don't provide enough relief, medications such as cimetidine
, ranitidine
, nizatidine
or famotidine
that help reduce the amount of acid the stomach produces are often prescribed. An even more effective way to limit stomach acid production is to shut down the acid "pumps" within acid-secreting stomach cells. Proton pump inhibitors reduce acid by blocking the action of these small pumps. This class of medications includes omeprazole
, lansoprazole
, rabeprazole
, and esomeprazole
. Proton pump inhibitors also appear to inhibit H. pylori activity. Cytoprotective agents are designed to help protect the tissues that line the stomach and small intestine. They include the medications sucralfate
and misoprostol
. If NSAIDs are being taken regularly, one of these medications to protect the stomach may also be taken. Another cytoprotective agent is bismuth subsalicylate
. Many people also drink milk as it helps protect the lining of the stomach and provides pain relief. In addition to protecting the lining of stomach and intestines, bismuth preparations appear to inhibit H. pylori activity as well. Several regimens are used to treat H. pylori infection. Most use a combination of two antibiotics and a proton pump inhibitor. Sometimes bismuth is also added to the regimen. The antibiotic aids in destroying the bacteria, and the acid blocker or proton pump inhibitor relieves pain and nausea, heals inflammation, and may increase the antibiotic's effectiveness.
Alcoholic beverage
An alcoholic beverage is a drink containing ethanol, commonly known as alcohol. Alcoholic beverages are divided into three general classes: beers, wines, and spirits. They are legally consumed in most countries, and over 100 countries have laws regulating their production, sale, and consumption...
consumption or prolonged use of nonsteroidal anti-inflammatory drugs (also known as NSAIDs) such as aspirin
Aspirin
Aspirin , also known as acetylsalicylic acid , is a salicylate drug, often used as an analgesic to relieve minor aches and pains, as an antipyretic to reduce fever, and as an anti-inflammatory medication. It was discovered by Arthur Eichengrun, a chemist with the German company Bayer...
or ibuprofen
Ibuprofen
Ibuprofen is a nonsteroidal anti-inflammatory drug used for relief of symptoms of arthritis, fever, as an analgesic , especially where there is an inflammatory component, and dysmenorrhea....
. Sometimes gastritis develops after major surgery, traumatic injury, burns, or severe infections. Gastritis may also occur in those who have had weight loss surgery resulting in the banding
Adjustable gastric band
A laparoscopic adjustable gastric band, commonly referred to as a lap band, is an inflatable silicone device that is placed around the top portion of the stomach, via laparoscopic surgery, in order to treat obesity...
or reconstruction of the digestive tract. Chronic causes are infection with bacteria, primarily Helicobacter pylori
Helicobacter pylori
Helicobacter pylori , previously named Campylobacter pyloridis, is a Gram-negative, microaerophilic bacterium found in the stomach. It was identified in 1982 by Barry Marshall and Robin Warren, who found that it was present in patients with chronic gastritis and gastric ulcers, conditions that were...
, chronic bile reflux
Biliary reflux
Biliary reflux or duodenogastric reflux is a condition that occurs when biliary fluid flows upward from the duodenum into the stomach and esophagus....
, stress and certain autoimmune disorders can cause gastritis as well. The most common symptom is abdominal upset or pain. Other symptoms are indigestion, abdominal bloating, nausea, and vomiting and pernicious anemia
Pernicious anemia
Pernicious anemia is one of many types of the larger family of megaloblastic anemias...
. Some may have a feeling of fullness or burning in the upper abdomen. A gastroscopy, blood test, complete blood count test, or a stool test may be used to diagnose gastritis. Treatment includes taking antacids or other medicines, such as proton pump inhibitors or antibiotics, and avoiding hot or spicy foods. For those with pernicious anemia
Pernicious anemia
Pernicious anemia is one of many types of the larger family of megaloblastic anemias...
, B12 injections are given.
Signs and symptoms
Abdominal pain
Abdominal pain can be one of the symptoms associated with transient disorders or serious disease. Making a definitive diagnosis of the cause of abdominal pain can be difficult, because many diseases can result in this symptom. Abdominal pain is a common problem...
is the most common symptom; the pain may be dull, vague, burning, aching, gnawing, sore, or sharp. Pain is usually located in the upper central portion of the abdomen, but it may occur anywhere from the upper left portion of the abdomen around to the back.
Other signs and symptoms may include:
- Nausea
- Vomiting (if present, may be clear, green or yellow, blood-streaked, or completely bloody, depending on the severity of the stomach inflammationInflammationInflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Inflammation is a protective attempt by the organism to remove the injurious stimuli and to initiate the healing process...
) - Belching (if present, usually does not relieve the pain much)
- BloatingBloatingBloating is any abnormal general swelling, or increase in diameter of the abdominal area. As a symptom, the patient feels a full and tight abdomen, which may cause abdominal pain sometimes accompanied by increased borborygmus or more seriously the total lack of borborygmus.-Symptoms:The most common...
- Feeling full after only a few bites of food
- Loss of appetite
- Unexplained weight loss
Acute
Erosive gastritis is a gastric mucosal erosion caused by damage to mucosal defenses. Alcohol consumption does not cause chronic gastritis. It does, however, erode the mucosal lining of the stomach; low doses of alcohol stimulate hydrochloric acidHydrochloric acid
Hydrochloric acid is a solution of hydrogen chloride in water, that is a highly corrosive, strong mineral acid with many industrial uses. It is found naturally in gastric acid....
secretion. High doses of alcohol do not stimulate secretion of acid. NSAIDs inhibit cyclooxygenase-1, or COX-1, an enzyme responsible for the biosynthesis of eicosanoids in the stomach, which increases the possibility of peptic ulcers forming. Also, NSAIDs, such as aspirin, reduce a substance that protects the stomach called prostaglandin
Prostaglandin
A prostaglandin is any member of a group of lipid compounds that are derived enzymatically from fatty acids and have important functions in the animal body. Every prostaglandin contains 20 carbon atoms, including a 5-carbon ring....
. These drugs used in a short period are not typically dangerous. However, regular use can lead to gastritis.
Chronic
Chronic gastritis refers to a wide range of problems of the gastric tissues that are the result of H. pylori infection. The immune system makes proteins and antibodies that fight infections in the body to maintain a homeostatic condition. In some disorders the body targets the stomach as if it were a foreign protein or pathogen; it makes antibodies against, severely damages, and may even destroy the stomach or its lining. In some cases bile, normally used to aid digestion in the small intestine, will enter through the pyloric valve of the stomach if it has been removed during surgery or does not work properly, also leading to gastritis. Gastritis may also be caused by other medical conditions, including HIV/AIDS, Crohn's diseaseCrohn's disease
Crohn's disease, also known as regional enteritis, is a type of inflammatory bowel disease that may affect any part of the gastrointestinal tract from mouth to anus, causing a wide variety of symptoms...
, certain connective tissue disorders, and liver or kidney failure.
Metaplasia
Mucous gland metaplasiaMetaplasia
Metaplasia is the reversible replacement of one differentiated cell type with another mature differentiated cell type. The change from one type of cell to another may generally be a part of normal maturation process or caused by some sort of abnormal stimulus...
, the reversible replacement of differentiated cells, occurs in the setting of severe damage of the gastric glands, which then waste away (atrophic gastritis
Atrophic gastritis
Atrophic gastritis is a process of chronic inflammation of the stomach mucosa, leading to loss of gastric glandular cells and their eventual replacement by intestinal and fibrous tissues...
), which are progressively replaced by mucous glands. Gastric ulcers may develop; it is unclear if they are the causes or the consequences. Intestinal metaplasia typically begins in response to chronic mucosal injury in the antrum
Antrum
In biology, antrum is a general term for a cavity or chamber which may have specific meaning in reference to certain organs or sites in the body.In vertebrates, it may mean for example:...
, and may extend to the body. Gastric mucosa cells change to resemble intestinal mucosa and may even assume absorptive characteristics. Intestinal metaplasia
Intestinal metaplasia
Intestinal metaplasia is the transformation of epithelium, usually of the stomach, to a type that bears some resemblance to the intestine. Initially, the transformed eptithelium bears resemblance to the small intestine; in the later stages, the epithelium resembles the colon...
is classified histologically as complete or incomplete. With complete metaplasia, gastric mucosa is completely transformed into small-bowel mucosa, both histologically and functionally, with the ability to absorb nutrients and secrete peptides. In incomplete metaplasia, the epithelium assumes a histologic appearance closer to that of the large intestine and frequently exhibits dysplasia.
Helicobacter pylori
Helicobacter pyloriHelicobacter pylori
Helicobacter pylori , previously named Campylobacter pyloridis, is a Gram-negative, microaerophilic bacterium found in the stomach. It was identified in 1982 by Barry Marshall and Robin Warren, who found that it was present in patients with chronic gastritis and gastric ulcers, conditions that were...
colonizes the stomach of more than half of the world's population, and the infection continues to play a key role in the pathogenesis of a number of gastroduodenal diseases. Colonization of the gastric mucosa with Helicobacter pylori results in the development of chronic gastritis in infected individuals and in a subset of patients chronic gastritis progresses to complications (i.e. ulcer disease, gastric neoplasias, some distinct extra gastric disorders). However, gastritis has no adverse consequences for most hosts and emerging evidence suggests that H. pylori prevalence is inversely related to gastroesophageal reflux disease
Gastroesophageal reflux disease
Gastroesophageal reflux disease , gastro-oesophageal reflux disease , gastric reflux disease, or acid reflux disease is chronic symptoms or mucosal damage caused by stomach acid coming up from the stomach into the esophagus...
and allergic disorders. These observations indicate that eradication may not be appropriate for certain populations due to the potentially beneficial effects conferred by persistent gastric inflammation.
Diagnosis
Often, a diagnosis can be made based on the patient's description of his or her symptoms, but other methods which may be used to verify gastritis include:- Blood tests:
- Blood cell count
- Presence of H. pylori
- Pregnancy
- Liver, kidney, gallbladder, or pancreas functions
- Urinalysis
- Stool sample, to look for blood in the stool
- X-rays
- ECGs
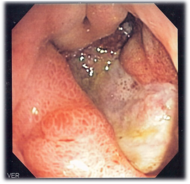
- Endoscopy, to check for stomach lining inflammation and mucous erosion
- Stomach biopsy, to test for gastritis and other conditions
Treatment
Over-the-counter antacids in liquid or tablet form are a common treatment for mild gastritis. Antacids neutralize stomach acid and can provide fast painPain
Pain is an unpleasant sensation often caused by intense or damaging stimuli such as stubbing a toe, burning a finger, putting iodine on a cut, and bumping the "funny bone."...
relief. When antacids don't provide enough relief, medications such as cimetidine
Cimetidine
Cimetidine INN is a histamine H2-receptor antagonist that inhibits the production of acid in the stomach. It is largely used in the treatment of heartburn and peptic ulcers. It is marketed by GlaxoSmithKline under the trade name Tagamet...
, ranitidine
Ranitidine
Ranitidine is a histamine H2-receptor antagonist that inhibits stomach acid production. It is commonly used in treatment of peptic ulcer disease and gastroesophageal reflux disease . Ranitidine is also used alongside fexofenadine and other antihistamines for the treatment of skin conditions...
, nizatidine
Nizatidine
Nizatidine is a histamine H2-receptor antagonist that inhibits stomach acid production, and commonly used in the treatment of peptic ulcer disease and gastroesophageal reflux disease...
or famotidine
Famotidine
Famotidine is a histamine H2-receptor antagonist that inhibits stomach acid production, and it is commonly used in the treatment of peptic ulcer disease and gastroesophageal reflux disease . It is commonly marketed by Johnson & Johnson/Merck under the trade names Pepcidine and Pepcid and by...
that help reduce the amount of acid the stomach produces are often prescribed. An even more effective way to limit stomach acid production is to shut down the acid "pumps" within acid-secreting stomach cells. Proton pump inhibitors reduce acid by blocking the action of these small pumps. This class of medications includes omeprazole
Omeprazole
Omeprazole is a proton pump inhibitor used in the treatment of dyspepsia, peptic ulcer disease , gastroesophageal reflux disease , laryngopharyngeal reflux and Zollinger–Ellison syndrome...
, lansoprazole
Lansoprazole
Lansoprazole is a proton-pump inhibitor which prevents the stomach from producing gastric acid. It is manufactured by a number of companies worldwide under several brand names . It was first approved by the U.S...
, rabeprazole
Rabeprazole
Rabeprazole is an antiulcer drug in the class of proton pump inhibitors. It was developed by Eisai Co. and is marketed by Janssen-Cilag as rabeprazole sodium under the brand names AcipHex in the US and Pariet in Britain, Italy, Greece, Australia, Brazil, Canada, Japan, and Russia. It is sold as...
, and esomeprazole
Esomeprazole
Esomeprazole is a proton pump inhibitor developed and marketed by AstraZeneca which is used in the treatment of dyspepsia, peptic ulcer disease , gastroesophageal reflux disease and Zollinger-Ellison syndrome...
. Proton pump inhibitors also appear to inhibit H. pylori activity. Cytoprotective agents are designed to help protect the tissues that line the stomach and small intestine. They include the medications sucralfate
Sucralfate
Sucralfate is a cytoprotective agent, an oral gastrointestinal medication primarily indicated for the treatment of active duodenal ulcers. Brand names include Sucramal in Italy; Carafate in U.S.A.; Pepsigard, Sucral, Sucrafil, Hapifate in India; Sutra or Musin in parts of South-East Asia; Sulcrate...
and misoprostol
Misoprostol
Misoprostol is a drug that is used for the prevention of non steroidal anti inflammatory drug induced gastric ulcers, for early abortion, to treat missed miscarriage, and to induce labor. The latter use is controversial in the United States. Misoprostol was invented and marketed by G.D...
. If NSAIDs are being taken regularly, one of these medications to protect the stomach may also be taken. Another cytoprotective agent is bismuth subsalicylate
Bismuth subsalicylate
Bismuth subsalicylate, with a nominal chemical formula of C7H5BiO4, It is a colloidal substance obtained by hydrolysis of bismuth salicylate . The actual structure is unknown and the formulation is only approximate. Recent evidence indicates that it is composed of a bismuth oxide core structure...
. Many people also drink milk as it helps protect the lining of the stomach and provides pain relief. In addition to protecting the lining of stomach and intestines, bismuth preparations appear to inhibit H. pylori activity as well. Several regimens are used to treat H. pylori infection. Most use a combination of two antibiotics and a proton pump inhibitor. Sometimes bismuth is also added to the regimen. The antibiotic aids in destroying the bacteria, and the acid blocker or proton pump inhibitor relieves pain and nausea, heals inflammation, and may increase the antibiotic's effectiveness.
See also
- StomachStomachThe stomach is a muscular, hollow, dilated part of the alimentary canal which functions as an important organ of the digestive tract in some animals, including vertebrates, echinoderms, insects , and molluscs. It is involved in the second phase of digestion, following mastication .The stomach is...
- GastroenteritisGastroenteritisGastroenteritis is marked by severe inflammation of the gastrointestinal tract involving both the stomach and small intestine resulting in acute diarrhea and vomiting. It can be transferred by contact with contaminated food and water...
- InfectionInfectionAn infection is the colonization of a host organism by parasite species. Infecting parasites seek to use the host's resources to reproduce, often resulting in disease...
- EsophagitisEsophagitisEsophagitis is inflammation of the esophagus. It may be acute or chronic. The acute esophagitis can be catarrhal or phlegmonous, whereas the chronic esophagitis may be hypertrophic or atrophic.-Infectious:...