

Estrogen
Encyclopedia

British English
British English, or English , is the broad term used to distinguish the forms of the English language used in the United Kingdom from forms used elsewhere...
), or œstrogens, are a group of compounds named for their importance in the estrous cycle
Estrous cycle
The estrous cycle comprises the recurring physiologic changes that are induced by reproductive hormones in most mammalian placental females. Estrous cycles start after puberty in sexually mature females and are interrupted by anestrous phases or pregnancies...
of humans and other animals. They are the primary female
Female
Female is the sex of an organism, or a part of an organism, which produces non-mobile ova .- Defining characteristics :The ova are defined as the larger gametes in a heterogamous reproduction system, while the smaller, usually motile gamete, the spermatozoon, is produced by the male...
sex hormones. Natural estrogens are steroid hormone
Steroid hormone
A steroid hormone is a steroid that acts as a hormone. Steroid hormones can be grouped into five groups by the receptors to which they bind: glucocorticoids, mineralocorticoids, androgens, estrogens, and progestogens...
s, while some synthetic ones are non-steroidal. Their name comes from the Greek words
Greek language
Greek is an independent branch of the Indo-European family of languages. Native to the southern Balkans, it has the longest documented history of any Indo-European language, spanning 34 centuries of written records. Its writing system has been the Greek alphabet for the majority of its history;...
estrus/οίστρος = sexual desire + gen/γόνο = to generate.
Estrogens are synthesized in all vertebrates as well as some insects. Their presence in both vertebrates and insects suggests that estrogenic sex hormones have an ancient evolutionary history.
Estrogens are used as part of some oral contraceptives, in estrogen replacement therapy for postmenopausal
Menopause
Menopause is a term used to describe the permanent cessation of the primary functions of the human ovaries: the ripening and release of ova and the release of hormones that cause both the creation of the uterine lining and the subsequent shedding of the uterine lining...
women, and in hormone replacement therapy
Hormone replacement therapy (male-to-female)
Hormone replacement therapy for transgender and transsexual people changes the balance of sex hormones in their bodies. Some intersex people also receive HRT, either starting in childhood to confirm the sex to which they were assigned, or later, if this assignment has proven to be incorrect...
for trans women.
Like all steroid hormones, estrogens readily diffuse
Diffusion
Molecular diffusion, often called simply diffusion, is the thermal motion of all particles at temperatures above absolute zero. The rate of this movement is a function of temperature, viscosity of the fluid and the size of the particles...
across the cell membrane
Cell membrane
The cell membrane or plasma membrane is a biological membrane that separates the interior of all cells from the outside environment. The cell membrane is selectively permeable to ions and organic molecules and controls the movement of substances in and out of cells. It basically protects the cell...
. Once inside the cell, they bind to and activate estrogen receptor
Estrogen receptor
Estrogen receptor refers to a group of receptors that are activated by the hormone 17β-estradiol . Two types of estrogen receptor exist: ER, which is a member of the nuclear hormone family of intracellular receptors, and the estrogen G protein-coupled receptor GPR30 , which is a G protein-coupled...
s which in turn modulate
Regulation of gene expression
Gene modulation redirects here. For information on therapeutic regulation of gene expression, see therapeutic gene modulation.Regulation of gene expression includes the processes that cells and viruses use to regulate the way that the information in genes is turned into gene products...
the expression
Gene expression
Gene expression is the process by which information from a gene is used in the synthesis of a functional gene product. These products are often proteins, but in non-protein coding genes such as ribosomal RNA , transfer RNA or small nuclear RNA genes, the product is a functional RNA...
of many gene
Gene
A gene is a molecular unit of heredity of a living organism. It is a name given to some stretches of DNA and RNA that code for a type of protein or for an RNA chain that has a function in the organism. Living beings depend on genes, as they specify all proteins and functional RNA chains...
s. Additionally, estrogens have been shown to activate a G protein-coupled receptor
G protein-coupled receptor
G protein-coupled receptors , also known as seven-transmembrane domain receptors, 7TM receptors, heptahelical receptors, serpentine receptor, and G protein-linked receptors , comprise a large protein family of transmembrane receptors that sense molecules outside the cell and activate inside signal...
, GPR30
GPR30
G-protein coupled estrogen receptor 1 also known as the membrane estrogen receptor or G-protein coupled receptor 30 is a G protein-coupled receptor that in humans is encoded by the GPER gene...
.
Steroidal
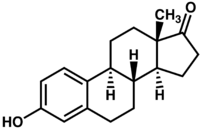
The three major naturally occurring estrogens in women are estroneEstrone
Estrone is an estrogenic hormone secreted by the ovary as well as adipose tissue.Estrone is one of several natural estrogens, which also include estriol and estradiol...
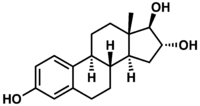
(E1), estradiol
Estradiol
Estradiol is a sex hormone. Estradiol is abbreviated E2 as it has 2 hydroxyl groups in its molecular structure. Estrone has 1 and estriol has 3 . Estradiol is about 10 times as potent as estrone and about 80 times as potent as estriol in its estrogenic effect...
(E2), and estriol
Estriol
Estriol is one of the three main estrogens produced by the human body.-Synthesis:Estriol is only produced in significant amounts during pregnancy as it is made by the placenta from 16-Hydroxydehydroepiandrosterone sulfate , an androgen steroid made in the fetal liver and adrenal glands.The human...
(E3).
Estrone is produced during menopause, estradiol is the predominant form in nonpregnant females, and estriol is the primary estrogen of pregnancy
Pregnancy
Pregnancy refers to the fertilization and development of one or more offspring, known as a fetus or embryo, in a woman's uterus. In a pregnancy, there can be multiple gestations, as in the case of twins or triplets...
. In the body these are all produced from androgen
Androgen
Androgen, also called androgenic hormone or testoid, is the generic term for any natural or synthetic compound, usually a steroid hormone, that stimulates or controls the development and maintenance of male characteristics in vertebrates by binding to androgen receptors...
s through actions of enzyme
Enzyme
Enzymes are proteins that catalyze chemical reactions. In enzymatic reactions, the molecules at the beginning of the process, called substrates, are converted into different molecules, called products. Almost all chemical reactions in a biological cell need enzymes in order to occur at rates...
s.
- From menarcheMenarcheMenarche is the first menstrual cycle, or first menstrual bleeding, in female human beings. From both social and medical perspectives it is often considered the central event of female puberty, as it signals the possibility of fertility....
to menopauseMenopauseMenopause is a term used to describe the permanent cessation of the primary functions of the human ovaries: the ripening and release of ova and the release of hormones that cause both the creation of the uterine lining and the subsequent shedding of the uterine lining...
the primary estrogen is estradiol. In postmenopausal women the primary estrogen is estrone. - The enzyme aromataseAromataseAromatase is an enzyme responsible for a key step in the biosynthesis of estrogens. It is a member of the cytochrome P450 superfamily , which are monooxygenases that catalyze many reactions involved in steroidogenesis. In particular, aromatase is responsible for the aromatization of androgens into...
converts testosteroneTestosteroneTestosterone is a steroid hormone from the androgen group and is found in mammals, reptiles, birds, and other vertebrates. In mammals, testosterone is primarily secreted in the testes of males and the ovaries of females, although small amounts are also secreted by the adrenal glands...
to estradiol. Aromatase also converts androstenedioneAndrostenedioneAndrostenedione is a 19-carbon steroid hormone produced in the adrenal glands and the gonads as an intermediate step in the biochemical pathway that produces the androgen testosterone and the estrogens estrone and estradiol.-Synthesis:Androstenedione is the common precursor of male and female sex...
to estrone. - Estrone is weaker than estradiol.
Premarin
Premarin
Premarin is the commercial name for a compound cream of vaginally administered estrogens, consisting primarily of conjugated estrogens. Isolated from mares' urine , it is manufactured by Wyeth Pharmaceuticals and has been marketed since 1942...
, a commonly prescribed estrogenic drug, contains the steroidal estrogens equilin
Equilin
Equilin is an estrogen from horses with the chemical name 3-hydroxyestra-1,3,5,7-tetraen-17-one. Equilin is one of the estrogens present in the mixture of estrogens isolated from horse urine and marketed as Premarin. Premarin became the most commonly used form of estrogen for hormone replacement...
and equilenin
Equilenin
Equilenin is a estrogenic steroid hormone obtained from the urine of pregnant mares. It is used as one of the components in Premarin.-External Links:**...
. There are oestradiol skin patches such as Estraderm (the original brand, introduced in the late 1980s) that offer a completely natural alternative. (A skin patch rather than pill also has the advantage of direct transmission into the blood stream without going through the liver.)
Nonsteroidal
A range of synthetic and natural substances have been identified that also possess estrogenic activity.- Synthetic substances of this kind are known as xenoestrogenXenoestrogenXenoestrogens are a type of xenohormone that imitates estrogen. They are widely used industrial compounds such as PCB, BPA and Phthalates, that have estrogenic effects on a living organism even though they differ chemically from the naturally occurring estrogenic substances internally produced by...
s. - Plant products with estrogenic activity are called phytoestrogens.
- Those produced by fungi are known as mycoestrogensMycoestrogensMycoestrogens are estrogens produced by fungi. The most important mycoestrogen is zearalenone, produced by Fusarium species of fungi. Zearalenone is the main phyto-oestrogen consumed in the USA. It may be one dietary factor that can reduce the prevalence of breast cancer.-In Food:Mycoestrogens...
.
Unlike estrogens produced by mammals, these substances are not necessarily steroids.
Biosynthesis
Ovarian follicle
Ovarian follicles are the basic units of female reproductive biology, each of which is composed of roughly spherical aggregations of cells found in the ovary. They contain a single oocyte . These structures are periodically initiated to grow and develop, culminating in ovulation of usually a single...
in the ovaries, the corpus luteum
Corpus luteum
The corpus luteum is a temporary endocrine structure in mammals, involved in production of relatively high levels of progesterone and moderate levels of estradiol and inhibin A...
, and the placenta
Placenta
The placenta is an organ that connects the developing fetus to the uterine wall to allow nutrient uptake, waste elimination, and gas exchange via the mother's blood supply. "True" placentas are a defining characteristic of eutherian or "placental" mammals, but are also found in some snakes and...
. Luteinizing hormone
Luteinizing hormone
Luteinizing hormone is a hormone produced by the anterior pituitary gland. In females, an acute rise of LH called the LH surge triggers ovulation and development of the corpus luteum. In males, where LH had also been called interstitial cell-stimulating hormone , it stimulates Leydig cell...
(LH) stimulates the production of estrogen in the ovaries
Ovary
The ovary is an ovum-producing reproductive organ, often found in pairs as part of the vertebrate female reproductive system. Ovaries in anatomically female individuals are analogous to testes in anatomically male individuals, in that they are both gonads and endocrine glands.-Human anatomy:Ovaries...
. Some estrogens are also produced in smaller amounts by other tissues such as the liver
Liver
The liver is a vital organ present in vertebrates and some other animals. It has a wide range of functions, including detoxification, protein synthesis, and production of biochemicals necessary for digestion...
, adrenal gland
Adrenal gland
In mammals, the adrenal glands are endocrine glands that sit atop the kidneys; in humans, the right suprarenal gland is triangular shaped, while the left suprarenal gland is semilunar shaped...
s, and the breast
Breast
The breast is the upper ventral region of the torso of a primate, in left and right sides, which in a female contains the mammary gland that secretes milk used to feed infants.Both men and women develop breasts from the same embryological tissues...
s. These secondary sources of estrogens are especially important in postmenopausal women. Fat cells
Adipocyte
However, in some reports and textbooks, the number of fat cell increased in childhood and adolescence. The total number is constant in both obese and lean adult...
also produce estrogen, potentially the reason why being underweight
Underweight
The term underweight refers to a human who is considered to be under a healthy weight. "Underweight" means weighing less than what is expected to be a healthy person . The definition is usually made with reference to the body mass index . A BMI of under 18.5 is usually referred to as underweight...
or overweight
Overweight
Overweight is generally defined as having more body fat than is optimally healthy. Being overweight is a common condition, especially where food supplies are plentiful and lifestyles are sedentary...
are risk factors for infertility
Infertility
Infertility primarily refers to the biological inability of a person to contribute to conception. Infertility may also refer to the state of a woman who is unable to carry a pregnancy to full term...
.
In females, synthesis of estrogens starts in theca interna
Theca interna
Theca interna cells express receptors for luteinizing hormone to produce androstenedione, which via a few steps, gives the granulosa the precursor for estrogen manufacturing....
cells in the ovary, by the synthesis of androstenedione
Androstenedione
Androstenedione is a 19-carbon steroid hormone produced in the adrenal glands and the gonads as an intermediate step in the biochemical pathway that produces the androgen testosterone and the estrogens estrone and estradiol.-Synthesis:Androstenedione is the common precursor of male and female sex...
from cholesterol
Cholesterol
Cholesterol is a complex isoprenoid. Specifically, it is a waxy steroid of fat that is produced in the liver or intestines. It is used to produce hormones and cell membranes and is transported in the blood plasma of all mammals. It is an essential structural component of mammalian cell membranes...
. Androstenedione is a substance of moderate androgenic activity. This compound crosses the basal membrane into the surrounding granulosa cell
Granulosa cell
A granulosa cell or follicular cell is a somatic cell of the sex cord that is closely associated with the developing female gamete in the ovary of mammals.-Anatomy and function:...
s, where it is converted to oestrone or oestradiol, either immediately or through testosterone. The conversion of testosterone to oestradiol, and of androstenedione to oestrone, is catalyzed by the enzyme aromatase
Aromatase
Aromatase is an enzyme responsible for a key step in the biosynthesis of estrogens. It is a member of the cytochrome P450 superfamily , which are monooxygenases that catalyze many reactions involved in steroidogenesis. In particular, aromatase is responsible for the aromatization of androgens into...
.
Oestradiol levels vary through the menstrual cycle, with levels highest just before ovulation
Ovulation
Ovulation is the process in a female's menstrual cycle by which a mature ovarian follicle ruptures and discharges an ovum . Ovulation also occurs in the estrous cycle of other female mammals, which differs in many fundamental ways from the menstrual cycle...
.
Function
The actions of estrogen are mediated by the Estrogen receptorEstrogen receptor
Estrogen receptor refers to a group of receptors that are activated by the hormone 17β-estradiol . Two types of estrogen receptor exist: ER, which is a member of the nuclear hormone family of intracellular receptors, and the estrogen G protein-coupled receptor GPR30 , which is a G protein-coupled...
(ER), a dimeric nuclear protein that binds to DNA and controls gene expression. Like other steroid hormones, estrogen enters passively into the cell where it binds to and activates the estrogen receptor. The estrogen:ER complex binds to specific DNA sequences called a Hormone response element
Hormone response element
A hormone response element is a response element for hormones, a short sequence of DNA within the promoter of a gene that is able to bind a specific hormone receptor complex and therefore regulate transcription...
to activate the transcription of some 137 ER-regulated genes, of which 89 are direct target genes. Since estrogen enters all cells, its action are dependent on the presence of the ER in the cell. The ER is expressed in specific tissues including the ovary, uterus and breast.
While estrogens are present in both men
Man
The term man is used for an adult human male . However, man is sometimes used to refer to humanity as a whole...
and women
Woman
A woman , pl: women is a female human. The term woman is usually reserved for an adult, with the term girl being the usual term for a female child or adolescent...
, they are usually present at significantly higher levels in women of reproductive age. They promote the development of female secondary sexual characteristics, such as breasts, and are also involved in the thickening of the endometrium
Endometrium
-Function:The endometrium is the innermost glandular layer and functions as a lining for the uterus, preventing adhesions between the opposed walls of the myometrium, thereby maintaining the patency of the uterine cavity. During the menstrual cycle or estrous cycle, the endometrium grows to a...
and other aspects of regulating the menstrual cycle
Menstrual cycle
The menstrual cycle is the scientific term for the physiological changes that can occur in fertile women for the purpose of sexual reproduction. This article focuses on the human menstrual cycle....
. In males, estrogen regulates certain functions of the reproductive system
Reproductive system
The reproductive system or genital system is a system of organs within an organism which work together for the purpose of reproduction. Many non-living substances such as fluids, hormones, and pheromones are also important accessories to the reproductive system. Unlike most organ systems, the sexes...
important to the maturation of sperm
Sperm
The term sperm is derived from the Greek word sperma and refers to the male reproductive cells. In the types of sexual reproduction known as anisogamy and oogamy, there is a marked difference in the size of the gametes with the smaller one being termed the "male" or sperm cell...
and may be necessary for a healthy libido. Furthermore, there are several other structural changes induced by estrogen in addition to other functions.
- Structural
- promote formation of female secondary sex characteristics
- accelerate metabolismMetabolismMetabolism is the set of chemical reactions that happen in the cells of living organisms to sustain life. These processes allow organisms to grow and reproduce, maintain their structures, and respond to their environments. Metabolism is usually divided into two categories...
- reduce muscleMuscleMuscle is a contractile tissue of animals and is derived from the mesodermal layer of embryonic germ cells. Muscle cells contain contractile filaments that move past each other and change the size of the cell. They are classified as skeletal, cardiac, or smooth muscles. Their function is to...
mass - increase fat stores
- stimulate endometrialEndometrium-Function:The endometrium is the innermost glandular layer and functions as a lining for the uterus, preventing adhesions between the opposed walls of the myometrium, thereby maintaining the patency of the uterine cavity. During the menstrual cycle or estrous cycle, the endometrium grows to a...
growth - increase uterineUterusThe uterus or womb is a major female hormone-responsive reproductive sex organ of most mammals including humans. One end, the cervix, opens into the vagina, while the other is connected to one or both fallopian tubes, depending on the species...
growth - increase vaginal lubricationVaginal lubricationVaginal lubrication is a lubricating fluid that is naturally produced in a woman's vagina. Vaginal lubrication or moistness is present at all times, but production increases significantly during a woman's sexual arousal in anticipation of sexual intercourse...
- thicken the vaginaVaginaThe vagina is a fibromuscular tubular tract leading from the uterus to the exterior of the body in female placental mammals and marsupials, or to the cloaca in female birds, monotremes, and some reptiles. Female insects and other invertebrates also have a vagina, which is the terminal part of the...
l wall - maintenance of vessel and skin
- reduce bone resorptionBone resorptionBone resorption is the process by which osteoclasts break down bone and release the minerals, resulting in a transfer of calcium from bone fluid to the blood....
, increase bone formation - morphic change (endomorphic -> mesomorphic -> ectomorphic)
- proteinProteinProteins are biochemical compounds consisting of one or more polypeptides typically folded into a globular or fibrous form, facilitating a biological function. A polypeptide is a single linear polymer chain of amino acids bonded together by peptide bonds between the carboxyl and amino groups of...
synthesis- increase hepatic production of binding proteinBinding proteinA binding protein is any protein that acts as an agent to bind two or more molecules together.Examples include:*DNA-binding protein**Single-strand binding protein**Telomere-binding protein*RNA-binding protein**Poly-binding protein...
s
- increase hepatic production of binding protein
- coagulationCoagulationCoagulation is a complex process by which blood forms clots. It is an important part of hemostasis, the cessation of blood loss from a damaged vessel, wherein a damaged blood vessel wall is covered by a platelet and fibrin-containing clot to stop bleeding and begin repair of the damaged vessel...
- increase circulating level of factors 2, 7Factor VIIFactor VII is one of the proteins that causes blood to clot in the coagulation cascade. It is an enzyme of the serine protease class. A recombinant form of human factor VIIa has U.S. Food and Drug Administration approval for uncontrolled bleeding in hemophilia patients...
, 9Factor IXFactor IX is one of the serine proteases of the coagulation system; it belongs to peptidase family S1. Deficiency of this protein causes hemophilia B. It was discovered in 1952 after a young boy named Stephen Christmas was found to be lacking this exact factor, leading to...
, 10Factor XFactor X, also known by the eponym Stuart-Prower factor or as prothrombinase, is an enzyme of the coagulation cascade. It is a serine endopeptidase .-Physiology:...
, plasminogen - decrease antithrombinAntithrombinAntithrombin is a small protein molecule that inactivates several enzymes of the coagulation system. Antithrombin is a glycoprotein produced by the liver and consists of 432 amino acids. It contains three disulfide bonds and a total of four possible glycosylation sites...
III - increase plateletPlateletPlatelets, or thrombocytes , are small,irregularly shaped clear cell fragments , 2–3 µm in diameter, which are derived from fragmentation of precursor megakaryocytes. The average lifespan of a platelet is normally just 5 to 9 days...
adhesiveness
- increase circulating level of factors 2, 7
- LipidLipidLipids constitute a broad group of naturally occurring molecules that include fats, waxes, sterols, fat-soluble vitamins , monoglycerides, diglycerides, triglycerides, phospholipids, and others...
- increase HDLHigh density lipoproteinHigh-density lipoprotein is one of the five major groups of lipoproteins, which, in order of sizes, largest to smallest, are chylomicrons, VLDL, IDL, LDL, and HDL, which enable lipids like cholesterol and triglycerides to be transported within the water-based bloodstream...
, triglycerideTriglycerideA triglyceride is an ester derived from glycerol and three fatty acids. There are many triglycerides, depending on the oil source, some are highly unsaturated, some less so.... - decrease LDLLow density lipoproteinLow-density lipoprotein is one of the five major groups of lipoproteins, which in order of size, largest to smallest, are chylomicrons, VLDL, IDL, LDL, and HDL, that enable transport of cholesterol within the water-based bloodstream...
, fatFatFats consist of a wide group of compounds that are generally soluble in organic solvents and generally insoluble in water. Chemically, fats are triglycerides, triesters of glycerol and any of several fatty acids. Fats may be either solid or liquid at room temperature, depending on their structure...
deposition
- increase HDL
- Fluid balance
- salt (sodiumSodiumSodium is a chemical element with the symbol Na and atomic number 11. It is a soft, silvery-white, highly reactive metal and is a member of the alkali metals; its only stable isotope is 23Na. It is an abundant element that exists in numerous minerals, most commonly as sodium chloride...
) and water retention - increase cortisolCortisolCortisol is a steroid hormone, more specifically a glucocorticoid, produced by the adrenal gland. It is released in response to stress and a low level of blood glucocorticoids. Its primary functions are to increase blood sugar through gluconeogenesis; suppress the immune system; and aid in fat,...
, SHBG
- salt (sodium
- Gastrointestinal tractGastrointestinal tractThe human gastrointestinal tract refers to the stomach and intestine, and sometimes to all the structures from the mouth to the anus. ....
- reduce bowel motility
- increase cholesterolCholesterolCholesterol is a complex isoprenoid. Specifically, it is a waxy steroid of fat that is produced in the liver or intestines. It is used to produce hormones and cell membranes and is transported in the blood plasma of all mammals. It is an essential structural component of mammalian cell membranes...
in bileBileBile or gall is a bitter-tasting, dark green to yellowish brown fluid, produced by the liver of most vertebrates, that aids the process of digestion of lipids in the small intestine. In many species, bile is stored in the gallbladder and upon eating is discharged into the duodenum...
- MelaninMelaninMelanin is a pigment that is ubiquitous in nature, being found in most organisms . In animals melanin pigments are derivatives of the amino acid tyrosine. The most common form of biological melanin is eumelanin, a brown-black polymer of dihydroxyindole carboxylic acids, and their reduced forms...
- increase pheomelanin, reduce eumelanin
- CancerCancerCancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
- support hormone-sensitive breast cancerBreast cancerBreast cancer is cancer originating from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the ducts with milk. Cancers originating from ducts are known as ductal carcinomas; those originating from lobules are known as lobular carcinomas...
s (see section below)
- support hormone-sensitive breast cancer
- Lung function
- promotes lung function by supporting alveoli (in rodents but probably in humans).
Sexual desire
Libido
Libido refers to a person's sex drive or desire for sexual activity. The desire for sex is an aspect of a person's sexuality, but varies enormously from one person to another, and it also varies depending on circumstances at a particular time. A person who has extremely frequent or a suddenly...
is dependent on androgen
Androgen
Androgen, also called androgenic hormone or testoid, is the generic term for any natural or synthetic compound, usually a steroid hormone, that stimulates or controls the development and maintenance of male characteristics in vertebrates by binding to androgen receptors...
levels rather than estrogen levels.
Fetal development
In mice, estrogens (which are locally aromatized from androgens in the brain) play an important role in psychosexual differentiation, for example, by masculinizing territorial behavior; the same is not true in humans. In humans, the masculinizing effects of prenatal androgens on behavior (and other tissues, with the possible exception of effects on bone) appear to act exclusively through the androgen receptor. As a result, the utility of rodent models for studying human psychosexual differentiation has been questioned.Mental health
Estrogen is considered to play a significant role in women’s mental healthMental health
Mental health describes either a level of cognitive or emotional well-being or an absence of a mental disorder. From perspectives of the discipline of positive psychology or holism mental health may include an individual's ability to enjoy life and procure a balance between life activities and...
. Sudden estrogen withdrawal, fluctuating estrogen, and periods of sustained estrogen low levels correlates with significant mood lowering. Clinical recovery from postpartum
Postnatal
Postnatal is the period beginning immediately after the birth of a child and extending for about six weeks. Another term would be postpartum period, as it refers to the mother...
, perimenopause, and postmenopause depression has been shown to be effective after levels of estrogen were stabilized and/or restored.
Low estrogen levels in male lab mice may be one cause of obsessive–compulsive disorder (OCD). When estrogen levels were raised through the increased activity of the enzyme aromatase
Aromatase
Aromatase is an enzyme responsible for a key step in the biosynthesis of estrogens. It is a member of the cytochrome P450 superfamily , which are monooxygenases that catalyze many reactions involved in steroidogenesis. In particular, aromatase is responsible for the aromatization of androgens into...
in male lab mice, OCD rituals were dramatically decreased. Hypothalamic
Hypothalamus
The Hypothalamus is a portion of the brain that contains a number of small nuclei with a variety of functions...
protein levels in the gene COMT
Catechol-O-methyl transferase
Catechol-O-methyltransferase is one of several enzymes that degrade catecholamines such as dopamine, epinephrine, and norepinephrine. In humans, catechol-O-methyltransferase protein is encoded by the COMT gene...
are enhanced by increasing estrogen levels which is believed to return mice that displayed OCD rituals to normal activity. Aromatase deficiency is ultimately suspected which is involved in the synthesis of estrogen in humans and has therapeutic implications in humans having obsessive-compulsive disorder.
Oral contraceptives
Since estrogen circulating in the blood can negatively feed-backNegative feedback
Negative feedback occurs when the output of a system acts to oppose changes to the input of the system, with the result that the changes are attenuated. If the overall feedback of the system is negative, then the system will tend to be stable.- Overview :...
to reduce circulating levels of FSH
Follicle-stimulating hormone
Follicle-stimulating hormone is a hormone found in humans and other animals. It is synthesized and secreted by gonadotrophs of the anterior pituitary gland. FSH regulates the development, growth, pubertal maturation, and reproductive processes of the body. FSH and Luteinizing hormone act...
and LH
Luteinizing hormone
Luteinizing hormone is a hormone produced by the anterior pituitary gland. In females, an acute rise of LH called the LH surge triggers ovulation and development of the corpus luteum. In males, where LH had also been called interstitial cell-stimulating hormone , it stimulates Leydig cell...
, most oral contraceptives contain a synthetic estrogen, along with a synthetic progestin
Progestin
A progestin is a synthetic progestogen that has progestinic effects similar to progesterone. The two most common uses of progestins are for hormonal contraception , and to prevent endometrial hyperplasia from unopposed estrogen in hormone replacement therapy...
. Even in men, the major hormone involved in LH feedback is estradiol
Estradiol
Estradiol is a sex hormone. Estradiol is abbreviated E2 as it has 2 hydroxyl groups in its molecular structure. Estrone has 1 and estriol has 3 . Estradiol is about 10 times as potent as estrone and about 80 times as potent as estriol in its estrogenic effect...
, not testosterone
Testosterone
Testosterone is a steroid hormone from the androgen group and is found in mammals, reptiles, birds, and other vertebrates. In mammals, testosterone is primarily secreted in the testes of males and the ovaries of females, although small amounts are also secreted by the adrenal glands...
.
Hormone replacement therapy
As more fully discussed in the article on Hormone replacement therapyHormone replacement therapy (menopause)
Hormone replacement therapy is a system of medical treatment for surgically menopausal, perimenopausal and to a lesser extent postmenopausal women...
, estrogen and other hormones are given to postmenopausal women in order to prevent osteoporosis
Osteoporosis
Osteoporosis is a disease of bones that leads to an increased risk of fracture. In osteoporosis the bone mineral density is reduced, bone microarchitecture is deteriorating, and the amount and variety of proteins in bone is altered...
as well as treat the symptoms of menopause such as hot flushes, vaginal dryness, urinary stress incontinence, chilly sensations, dizziness, fatigue, irritability, and sweating. Fractures of the spine, wrist, and hips decrease by 50-70% and spinal bone density increases by ~5% in those women treated with estrogen within 3 years of the onset of menopause and for 5–10 years thereafter.
Before the specific dangers of conjugated equine estrogens were well understood, standard therapy was 0.625 mg/day of conjugated equine estrogens (such as Premarin). There are, however, risks associated with conjugated equine estrogen therapy. Among the older postmenopausal women studied as part of the Women's Health Initiative
Women's Health Initiative
The Women's Health Initiative was initiated by the U.S. National Institutes of Health in 1991. The objective of this women's health research initiative was to conduct medical research into some of the major health problems of older women...
(WHI), an orally administered conjugated equine estrogen supplement was found to be associated with an increased risk of dangerous blood clotting. The WHI studies used one type of estrogen supplement, a high oral dose of conjugated equine estrogens (Premarin
Premarin
Premarin is the commercial name for a compound cream of vaginally administered estrogens, consisting primarily of conjugated estrogens. Isolated from mares' urine , it is manufactured by Wyeth Pharmaceuticals and has been marketed since 1942...
alone and with medroxyprogesterone acetate as PremPro).
In a study by the NIH, esterified estrogens were not proven to pose the same risks to health as conjugated equine estrogens. Hormone replacement therapy
Hormone replacement therapy (menopause)
Hormone replacement therapy is a system of medical treatment for surgically menopausal, perimenopausal and to a lesser extent postmenopausal women...
has favorable effects on serum cholesterol levels, and when initiated immediately upon menopause may reduce the incidence of cardiovascular disease, although this hypothesis has yet to be tested in randomized trials. Estrogen appears to have a protector effect on atherosclerosis : it lowers LDL and triglycerides, it raises HDL levels and has endothelial vasodilatation properties plus an anti-inflammatory component.
Research is underway to determine if risks of estrogen supplement use are the same for all methods of delivery. In particular, estrogen applied topical
Topical
In medicine, a topical medication is applied to body surfaces such as the skin or mucous membranes such as the vagina, anus, throat, eyes and ears.Many topical medications are epicutaneous, meaning that they are applied directly to the skin...
ly may have a different spectrum of side-effects than when administered orally, and transdermal estrogens do not affect clotting as they are absorbed directly into the systemic circulation, avoiding first-pass metabolism in the liver. This route of administration is thus preferred in women with a history of thrombo-embolic disease.
Estrogen is also used in the therapy of vaginal atrophy, hypoestrogenism (as a result of hypogonadism, castration, or primary ovarian failure), amenorrhea, dysmenorrhea, and oligomenorrhea. Estrogens can also be used to suppress lactation
Lactation
Lactation describes the secretion of milk from the mammary glands and the period of time that a mother lactates to feed her young. The process occurs in all female mammals, however it predates mammals. In humans the process of feeding milk is called breastfeeding or nursing...
after child birth.
Breast cancer
About 80% of breast cancers, once established, rely on supplies of the hormone estrogen to grow: they are known as hormone-sensitive or hormone-receptor-positive cancers. Suppression of production of estrogen in the body is a treatment for these cancers.Recently researchers have discovered that the common table mushroom has anti-aromatase
Aromatase
Aromatase is an enzyme responsible for a key step in the biosynthesis of estrogens. It is a member of the cytochrome P450 superfamily , which are monooxygenases that catalyze many reactions involved in steroidogenesis. In particular, aromatase is responsible for the aromatization of androgens into...
properties and therefore possible anti-estrogen activity. Clinical trials have begun in the United States
United States
The United States of America is a federal constitutional republic comprising fifty states and a federal district...
looking into whether the table mushroom can prevent breast cancer in people. A recent study has highlighted the importance of this research. In 2009, a case-control study of the eating habits of 2,018 women, revealed that women who consumed mushrooms had an approximately 50% lower incidence of breast cancer
Breast cancer
Breast cancer is cancer originating from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the ducts with milk. Cancers originating from ducts are known as ductal carcinomas; those originating from lobules are known as lobular carcinomas...
. Women who consumed mushrooms and green tea
Green tea
Green tea is made solely from the leaves of Camellia sinensis that have undergone minimal oxidation during processing. Green tea originates from China and has become associated with many cultures throughout Asia. It has recently become more widespread in the West, where black tea is traditionally...
had a 90% lower incidence of breast cancer
Breast cancer
Breast cancer is cancer originating from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the ducts with milk. Cancers originating from ducts are known as ductal carcinomas; those originating from lobules are known as lobular carcinomas...
.
Hormone-receptor-positive breast cancers are treated with drugs which suppress production of estrogen in the body. This technique, in the context of treatment of breast cancer, is known variously as hormonal therapy, hormone therapy, or anti-estrogen therapy (not to be confused with hormone replacement therapy). Certain foods such as soy may also suppress the proliferative effects of estrogen and are used as an alternative to hormone therapy.
Prostate cancer
Under certain circumstances, estrogen may also be used in males for treatment of prostate cancerProstate cancer
Prostate cancer is a form of cancer that develops in the prostate, a gland in the male reproductive system. Most prostate cancers are slow growing; however, there are cases of aggressive prostate cancers. The cancer cells may metastasize from the prostate to other parts of the body, particularly...
.
Miscellaneous
In humans and mice, estrogen promotes wound healing.At one time, estrogen was used to induce growth attenuation
Growth attenuation
Growth attenuation is an elective medical treatment which involves administering estrogen to cause closure of the epiphyses of the bones , resulting in a reduced adult height. Since the 1960s this treatment has been performed primarily on children growing toward an adult height considered...
in tall girls. Recently, estrogen-induced growth attenuation was used as part of the controversial Ashley Treatment
Ashley Treatment
The Ashley Treatment refers to a controversial set of medical procedures undergone by a Seattle child, "Ashley X". Ashley, born in 1997, has severe developmental disabilities due to static encephalopathy of unknown etiology; she is, and will remain, at an infant level mentally and physically...
to keep a developmentally disabled girl from growing to adult size.
Most recently, estrogen has been used in experimental research as a way to treat patients suffering from bulimia nervosa
Bulimia nervosa
Bulimia nervosa is an eating disorder characterized by binge eating and purging or consuming a large amount of food in a short amount of time, followed by an attempt to rid oneself of the food consumed, usually by purging and/or by laxative, diuretics or excessive exercise. Bulimia nervosa is...
, in addition to Cognitive Behavioral Therapy, which is the established standard for treatment in bulimia cases. The estrogen research hypothesizes that the disease may be linked to a hormonal imbalance in the brain.
Estrogen has also been used in studies which indicate that it may be an effective drug for use in the treatment of traumatic liver injury.
Health risks and warning labels
Hyperestrogenemia (elevated levels of estrogen) may be a result of exogenous administration of estrogen or estrogen-like substances, or may be a result of physiologic conditions such as pregnancy. Any of these causes is linked with an increase in the risk of thrombosisThrombosis
Thrombosis is the formation of a blood clot inside a blood vessel, obstructing the flow of blood through the circulatory system. When a blood vessel is injured, the body uses platelets and fibrin to form a blood clot to prevent blood loss...
.
The estrogen-alone substudy of the WHI reported an increased risk of stroke
Stroke
A stroke, previously known medically as a cerebrovascular accident , is the rapidly developing loss of brain function due to disturbance in the blood supply to the brain. This can be due to ischemia caused by blockage , or a hemorrhage...
and deep vein thrombosis
Deep vein thrombosis
Deep vein thrombosis is the formation of a blood clot in a deep vein. Deep vein thrombosis commonly affects the leg veins or the deep veins of the pelvis. Occasionally the veins of the arm are affected...
(DVT) in postmenopausal women 50 years of age or older and an increased risk of dementia
Dementia
Dementia is a serious loss of cognitive ability in a previously unimpaired person, beyond what might be expected from normal aging...
in postmenopausal women 65 years of age or older using 0.625 mg of Premarin conjugated equine estrogens (CEE). The estrogen-plus-progestin substudy of the WHI reported an increased risk of myocardial infarction
Myocardial infarction
Myocardial infarction or acute myocardial infarction , commonly known as a heart attack, results from the interruption of blood supply to a part of the heart, causing heart cells to die...
, stroke, invasive breast cancer, pulmonary emboli and DVT in postmenopausal women 50 years of age or older and an increased risk of dementia in postmenopausal women 65 years of age or older using PremPro, which is 0.625 mg of CEE with 2.5 mg of the progestin medroxyprogesterone acetate (MPA).
The labeling of estrogen-only products in the U.S. includes a boxed warning
Black box warning
In the United States, a black box warning is a type of warning that appears on the package insert for prescription drugs that may cause serious adverse effects...
that unopposed estrogen (without progestagen
Progestagen
Progestogens are a group of hormones including progesterone.The progestogens are one of the five major classes of steroid hormones, in addition to the estrogens, androgens, mineralocorticoids, and glucocorticoids. All progestogens are characterized by their basic 21-carbon skeleton, called a...
) therapy increases the risk of endometrial cancer
Endometrial cancer
Endometrial cancer refers to several types of malignancies that arise from the endometrium, or lining, of the uterus. Endometrial cancers are the most common gynecologic cancers in the United States, with over 35,000 women diagnosed each year. The incidence is on a slow rise secondary to the...
. Based on a review of data from the WHI, on January 8, 2003 the FDA changed the labeling of all estrogen and estrogen with progestin products for use by postmenopausal women to include a new boxed warning about cardiovascular and other risks.
Cosmetics
Some hair shampooShampoo
Shampoo is a hair care product used for the removal of oils, dirt, skin particles, dandruff, environmental pollutants and other contaminant particles that gradually build up in hair...
s on the market include estrogens and placental extracts; others contain phytoestrogens. There are case reports of young children developing breasts after exposure to these shampoos.
On September 9, 1993, the FDA determined that not all topically applied hormone-containing drug products for OTC
Over-the-counter drug
Over-the-counter drugs are medicines that may be sold directly to a consumer without a prescription from a healthcare professional, as compared to prescription drugs, which may be sold only to consumers possessing a valid prescription...
human use are generally recognized as safe and effective
Generally recognized as safe and effective
Generally recognized as safe and effective is a legal term used to describe certain old drugs that do not require prior approval from the U.S...
and are misbranded. An accompanying proposed rule deals with cosmetics, concluding that any use of natural estrogens in a cosmetic product makes the product an unapproved new drug and that any cosmetic using the term "hormone" in the text of its labeling or in its ingredient statement makes an implied drug claim, subjecting such a product to regulatory action.
In addition to being considered misbranded drugs, products claiming to contain placental extract may also be deemed to be misbranded cosmetics if the extract has been prepared from placentas from which the hormones and other biologically active substances have been removed and the extracted substance consists principally of protein. The FDA recommends that this substance be identified by a name other than "placental extract" and describing its composition more accurately because consumers associate the name "placental extract" with a therapeutic use of some biological activity.
History
In 1929 Adolf ButenandtAdolf Butenandt
Adolf Friedrich Johann Butenandt was a German biochemist and member of the Nazi party. He was awarded the Nobel Prize in Chemistry in 1939 for his "work on sex hormones." He initially rejected the award in accordance with government policy, but accepted it in 1949 after World War...
and Edward Adelbert Doisy
Edward Adelbert Doisy
Edward Adelbert Doisy was an American biochemist. He received the Nobel Prize in Physiology or Medicine in 1943 with Henrik Dam for their discovery of vitamin K and its chemical structure.Doisy was born in Hume, Illinois, on November 3, 1893. He completed his A.B. degree in 1914 and his M.S...
independently isolated and determined the structure of estrogen. Thereafter, the market for hormonal drug research opened up.
The “first orally effective estrogen”, Emmenin, derived from the late-pregnancy urine of Canadian women, was introduced in 1930 by Collip and Ayerst Laboratories. Estrogens are not water-soluble and cannot be given orally, but the urine was found to contain estriol glucuronide
Glucuronide
A glucuronide, also known as glucuronoside, is any substance produced by linking glucuronic acid to another substance via a glycosidic bond...
which is water soluble and becomes active in the body after hydrolization.
Scientists continued to search for new sources of estrogen because of concerns associated with the practicality of introducing the drug into the market. At the same time, a German pharmaceutical drug company, formulated a similar product as Emmenin that was introduced to German women to treat menopausal symptoms.
In 1938, British scientists obtained a patent on a newly formulated nonsteroidal estrogen, diethylstilbestrol
Diethylstilbestrol
Diethylstilbestrol is a synthetic nonsteroidal estrogen that was first synthesized in 1938. Human exposure to DES occurred through diverse sources, such as dietary ingestion from supplemented cattle feed and medical treatment for certain conditions, including breast and prostate cancers...
(DES), that was cheaper and more powerful than the previously manufactured estrogens. Soon after, concerns over the side effects of DES were raised in scientific journals while the drug manufacturers came together to lobby for governmental approval of DES. It was only until 1941 when estrogen therapy was finally approved by the Food and Drug Administration (FDA) for the treatment of menopausal symptoms.
Environmental effects
Estrogens are among the wide range of endocrine-disrupting compounds (EDCsEndocrine disruptor
Endocrine disruptors are chemicals that interfere with endocrine in animals, including humans. These disruptions can cause cancerous tumors, birth defects, and other developmental disorders...
) because they have high estrogenic potency. When this specific EDC makes its way into the environment it may cause male reproductive dysfunction to wildlife. The estrogen excreted from farm animals makes its way into fresh water systems. During the germination period of reproduction the fish are exposed to low levels of estrogen which may cause reproductive dysfunction to male fish.
See also
External links
- It's wise to be wary of the pill
- Nussey and Whitehead: Endocrinology, an integrated approach, Taylor and Francis 2001. Free online textbook.