
Episiotomy
Encyclopedia
An episiotomy also known as perineotomy, is a surgically planned incision on the perineum
and the posterior vaginal wall during second stage of labor. The incision, which can be midline or at an angle from the posterior end of the vulva
, is performed under local anaesthetic (pudendal anesthesia
), and is sutured closed after delivery. It is one of the most common medical procedures performed on women, and although its routine use in childbirth has steadily declined in recent decades, it is still widely practiced in many parts of the world including Latin America
, Poland
, Bulgaria
, India
and Taiwan.
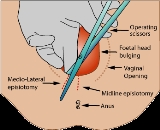
Though indications on the need for episiotomy vary, and may even be controversial (see discussion below), where the technique is applied, there are two main variations. Both are depicted in the above image. In one variation, the midline episiotomy, the line of incision is central over the anus. This technique bifurcates the perineal body
, which is essential for the integrity of the pelvic floor. Precipitous birth can also sever - and more severely sever - the perineal body, leading to undesired birth sequelae such as incontinence. Therefore, the oblique technique is often applied (also pictured above). In the oblique technique, the perineal body is avoided, cutting only the vagina epithelium, skin and muscles (transversalius and bulbospongiosus). This technique aids in avoiding trauma to the perineal body by either surgical or traumatic means.
In 2009, a Cochrane meta-analysis based on studies with over 5000 women concluded that: "Restrictive episiotomy policies appear to have a number of benefits compared to policies based on routine episiotomy. There is less posterior perineal trauma, less suturing and fewer complications, no difference for most pain measures and severe vaginal or perineal trauma, but there was an increased risk of anterior perineal trauma with restrictive episiotomy." The authors were unable to find any good quality studies that compared mediolateral versus midline episiotomy.
by reducing anal sphincter muscle damage, reduce the loss of blood
during delivery, and protect against neonatal trauma. While episiotomy is employed to obviate issues such as post-partum pain, incontinence and sexual dysfunction, some studies suggest that in actuality, episiotomy surgery itself can cause all of these problems. Research has shown that natural tears typically are less severe (although this is perhaps not surprising since an episiotomy is designed for when natural tearing will cause significant risks or trauma). Slow delivery of the head in between contractions will result in the least perineal damage. Studies in 2010 based on interviews with postpartum women have concluded that limiting perineal trauma during birth is conducive to continued sexual function after birth. At least one study has recommended that routine episiotomy be abandoned for this reason.
In various countries, routine episiotomy has been accepted medical practice for many years.
Since about the 1960s, routine episiotomies have been rapidly losing popularity among obstetricians and midwives in Europe, Australia and the United States. A nationwide US population study suggested that 31% of women having babies in U.S. hospitals received episiotomies in 1997, compared with 56% in 1979. In Latin America
it remains popular, and is performed in 90% of hospital births, in most cases without the mother's consent [Citation Needed].
, particularly in midline episiotomies. In addition it may complicate sexual intercourse
by making it painful and replacing erectile tissue
s in the vulva with fibrotic tissue.
In cases where an episiotomy is indicated, a mediolateral incision may be preferable to a median (midline) incision, as the latter is associated with a higher risk of injury to the anal sphincter and the rectum.
Perineal massage
beginning around the 34th week has been shown to reduce perineal damage by 6%.
A perineal dilator
can be used to stretch the perineal tissue gradually and train it in preparation for first births. The "Epi-no Birth Trainer" consists of a small inflatable silicone balloon pumped with the same pump as a sphygmomanometer
. The Epi-no device has been shown to reduce perineal damage by 50% at first births.
Where episiotomy is never practiced, the sutured tear rates for first birth were documented to be about 30%. Among 104 consecutive primiparous women who practiced with an Epi-No birth trainer before birth and had normal vaginal births, 10% had sutured perineums. Neither group suffered any third- or fourth-degree tears. The average birthweight was 3,400 g. This 10% rate of sutured perineums among first births who used EPINO birth trainer is the lowest reported for healthy primiparous women to date.
Perineum
In human anatomy, the perineum is a region of the body including the perineal body and surrounding structures...
and the posterior vaginal wall during second stage of labor. The incision, which can be midline or at an angle from the posterior end of the vulva
Vulva
The vulva consists of the external genital organs of the female mammal. This article deals with the vulva of the human being, although the structures are similar for other mammals....
, is performed under local anaesthetic (pudendal anesthesia
Pudendal anesthesia
Pudendal anesthesia, also known as a pudendal block, is a form of local anesthesia commonly used in the practice of obstetrics to relieve pain during pregnancy. The anesthesia is produced by blocking the pudendal nerves near the ischial spine of the pelvis...
), and is sutured closed after delivery. It is one of the most common medical procedures performed on women, and although its routine use in childbirth has steadily declined in recent decades, it is still widely practiced in many parts of the world including Latin America
Latin America
Latin America is a region of the Americas where Romance languages – particularly Spanish and Portuguese, and variably French – are primarily spoken. Latin America has an area of approximately 21,069,500 km² , almost 3.9% of the Earth's surface or 14.1% of its land surface area...
, Poland
Poland
Poland , officially the Republic of Poland , is a country in Central Europe bordered by Germany to the west; the Czech Republic and Slovakia to the south; Ukraine, Belarus and Lithuania to the east; and the Baltic Sea and Kaliningrad Oblast, a Russian exclave, to the north...
, Bulgaria
Bulgaria
Bulgaria , officially the Republic of Bulgaria , is a parliamentary democracy within a unitary constitutional republic in Southeast Europe. The country borders Romania to the north, Serbia and Macedonia to the west, Greece and Turkey to the south, as well as the Black Sea to the east...
, India
India
India , officially the Republic of India , is a country in South Asia. It is the seventh-largest country by geographical area, the second-most populous country with over 1.2 billion people, and the most populous democracy in the world...
and Taiwan.
Uses
Episiotomy is done as prophylaxis against soft-tissue-trauma. Vaginal tears can occur during childbirth, most often at the vaginal opening as the baby's head passes through, especially if the baby descends quickly. Tears can involve the perineal skin or extend to the muscles and the anal sphincter and anus. The midwife or obstetrician may decide to make a surgical cut to the perineum with scissors or scalpel (episiotomy) to make the baby's birth easier and prevent severe tears that can be difficult to repair. The cut is repaired with stitches (sutures). Some childbirth facilities have a policy of routine episiotomy.Though indications on the need for episiotomy vary, and may even be controversial (see discussion below), where the technique is applied, there are two main variations. Both are depicted in the above image. In one variation, the midline episiotomy, the line of incision is central over the anus. This technique bifurcates the perineal body
Perineal body
The perineal body is a pyramidal fibromuscular mass in the middle line of the perineum at the junction between the urogenital triangle and the anal triangle . It is found in both males and females...
, which is essential for the integrity of the pelvic floor. Precipitous birth can also sever - and more severely sever - the perineal body, leading to undesired birth sequelae such as incontinence. Therefore, the oblique technique is often applied (also pictured above). In the oblique technique, the perineal body is avoided, cutting only the vagina epithelium, skin and muscles (transversalius and bulbospongiosus). This technique aids in avoiding trauma to the perineal body by either surgical or traumatic means.
In 2009, a Cochrane meta-analysis based on studies with over 5000 women concluded that: "Restrictive episiotomy policies appear to have a number of benefits compared to policies based on routine episiotomy. There is less posterior perineal trauma, less suturing and fewer complications, no difference for most pain measures and severe vaginal or perineal trauma, but there was an increased risk of anterior perineal trauma with restrictive episiotomy." The authors were unable to find any good quality studies that compared mediolateral versus midline episiotomy.
Indications
- There is a serious risk to the mother of second or third degree tearing
- In cases where a natural delivery is adversely affected, but a Caesarean sectionCaesarean sectionA Caesarean section, is a surgical procedure in which one or more incisions are made through a mother's abdomen and uterus to deliver one or more babies, or, rarely, to remove a dead fetus...
is not indicated - 'Natural' tearing will cause an increased risk of maternal disease being vertically transmitted
- The baby is very large
- When perineal muscles are excessively rigid
- When instrumental delivery is indicated
- When a woman has undergone FGM (female genital mutilation), indicating the need for an anterior and or mediolateral episiotomy
- Prolonged late decelerations or fetal bradycardiaBradycardiaBradycardia , in the context of adult medicine, is the resting heart rate of under 60 beats per minute, though it is seldom symptomatic until the rate drops below 50 beat/min. It may cause cardiac arrest in some patients, because those with bradycardia may not be pumping enough oxygen to their heart...
during active pushing - The baby's shoulders are stuck (shoulder dystociaShoulder dystociaShoulder dystocia is a specific case of dystocia whereby after the delivery of the head, the anterior shoulder of the infant cannot pass below the pubic symphysis, or requires significant manipulation to pass below the pubic symphysis. It is diagnosed when the shoulders fail to deliver shortly...
), or a bony association (Note that the episiotomy does not directly resolve this problem, but it is indicated to allow the operator more room to perform maneuvers to free shoulders from the pelvis)
Types
There are four main types of episiotomy:- Medio-lateral: The incision is made downward and outward from midpoint of fourchette either to right or left. It is directed diagonally in straight line which runs about 2.5 cm away from the anus (midpoint between anus and ischial tuberosity).
- Median: The incision commences from center of the fourchette and extends on posterios side along midline for 2.5 cm.
- Lateral: The incision starts from about 1 cm away from the center of fourchette and extends laterally. Drawback include chance of injury to Bartholin's ductBartholin's ductBartholin's ducts are a pair of ducts leading from the Bartholin's glands to the surface of the vulva.It is claimed that the two external openings of the Bartholin's ducts are often invisible to the naked human eye....
. Thus some practiotioners have totally condemned it. - 'J' shaped: The incision begins in the center of the fourchette and is directed posteriorly along midline for about 1.5 cm and then directed downwards and outwards along 5 or 7 o'clock position to avoid the anal sphincter. This is also not done widely.
Controversy about common usage and history of the technique
Traditionally, physicians have used episiotomies in an effort to lessen perineal trauma, minimize postpartum pelvic floor dysfunctionPostpartum pelvic floor dysfunction
Pelvic floor dysfunction refers to a wide range of issues that occur when muscles of the pelvic floor are weak, tight, or there is an impairment of the sacroiliac joint, lower back, coccyx, or hip joints. Tissues surrounding the pelvic organs may have increased or decreased sensitivity or...
by reducing anal sphincter muscle damage, reduce the loss of blood
Blood
Blood is a specialized bodily fluid in animals that delivers necessary substances such as nutrients and oxygen to the cells and transports metabolic waste products away from those same cells....
during delivery, and protect against neonatal trauma. While episiotomy is employed to obviate issues such as post-partum pain, incontinence and sexual dysfunction, some studies suggest that in actuality, episiotomy surgery itself can cause all of these problems. Research has shown that natural tears typically are less severe (although this is perhaps not surprising since an episiotomy is designed for when natural tearing will cause significant risks or trauma). Slow delivery of the head in between contractions will result in the least perineal damage. Studies in 2010 based on interviews with postpartum women have concluded that limiting perineal trauma during birth is conducive to continued sexual function after birth. At least one study has recommended that routine episiotomy be abandoned for this reason.
In various countries, routine episiotomy has been accepted medical practice for many years.
Since about the 1960s, routine episiotomies have been rapidly losing popularity among obstetricians and midwives in Europe, Australia and the United States. A nationwide US population study suggested that 31% of women having babies in U.S. hospitals received episiotomies in 1997, compared with 56% in 1979. In Latin America
Latin America
Latin America is a region of the Americas where Romance languages – particularly Spanish and Portuguese, and variably French – are primarily spoken. Latin America has an area of approximately 21,069,500 km² , almost 3.9% of the Earth's surface or 14.1% of its land surface area...
it remains popular, and is performed in 90% of hospital births, in most cases without the mother's consent [Citation Needed].
Discussion
Having an episiotomy may increase perineal pain during postpartum recovery, resulting in trouble defecatingDefecation
Defecation is the final act of digestion by which organisms eliminate solid, semisolid or liquid waste material from the digestive tract via the anus. Waves of muscular contraction known as peristalsis in the walls of the colon move fecal matter through the digestive tract towards the rectum...
, particularly in midline episiotomies. In addition it may complicate sexual intercourse
Sexual intercourse
Sexual intercourse, also known as copulation or coitus, commonly refers to the act in which a male's penis enters a female's vagina for the purposes of sexual pleasure or reproduction. The entities may be of opposite sexes, or they may be hermaphroditic, as is the case with snails...
by making it painful and replacing erectile tissue
Erectile tissue
Erectile tissue is tissue in the body that can become erect, usually by becoming engorged with blood.-Erectile tissue in the clitoris and penis:...
s in the vulva with fibrotic tissue.
In cases where an episiotomy is indicated, a mediolateral incision may be preferable to a median (midline) incision, as the latter is associated with a higher risk of injury to the anal sphincter and the rectum.
Impacts on sexual intercourse
Some midwives compare routine episiotomy to female circumcision. One study found that women who underwent episiotomy reported more painful intercourse and insufficient lubrication 12–18 months after birth, but did not find any problems with orgasm or arousal.Lessening the Need for Episiotomy
Controlled delivery of the head that allows slow gradual stretching of the perineal tissue can help in minimizing damage to the perineum.Perineal massage
Perineal massage
Perineal massage is the practice of massaging a pregnant woman's perineum around the vagina in preparation for childbirth. The intention is to attempt to prevent tearing of the perineum during birth, the need for an episiotomy or an instrument delivery.Randomized clinical trials of perineal...
beginning around the 34th week has been shown to reduce perineal damage by 6%.
A perineal dilator
Perineal dilator
A perineal dilator is an inflatable bubble-like device used to prepare women for the experience of childbirth. The device, usually made out of silicone, is inserted into the vagina and inflated, and then pushed out. Use of the device allows gradual stretching of the perineum in order to prevent...
can be used to stretch the perineal tissue gradually and train it in preparation for first births. The "Epi-no Birth Trainer" consists of a small inflatable silicone balloon pumped with the same pump as a sphygmomanometer
Sphygmomanometer
A sphygmomanometer or blood pressure meter is a device used to measure blood pressure, comprising an inflatable cuff to restrict blood flow, and a mercury or mechanical manometer to measure the pressure. It is always used in conjunction with a means to determine at what pressure blood flow is just...
. The Epi-no device has been shown to reduce perineal damage by 50% at first births.
Where episiotomy is never practiced, the sutured tear rates for first birth were documented to be about 30%. Among 104 consecutive primiparous women who practiced with an Epi-No birth trainer before birth and had normal vaginal births, 10% had sutured perineums. Neither group suffered any third- or fourth-degree tears. The average birthweight was 3,400 g. This 10% rate of sutured perineums among first births who used EPINO birth trainer is the lowest reported for healthy primiparous women to date.