

Coenzyme Q
Encyclopedia
Coenzyme Q10, also known as ubiquinone, ubidecarenone, coenzyme Q, and abbreviated at times to CoQ10 ˌkoʊ ˌkjuː ˈtɛn, CoQ, Q10, or Q, is a 1,4-benzoquinone
, where Q refers to the quinone
chemical group, and 10 refers to the number of isoprenyl
chemical subunits in its tail.
This oil-soluble, vitamin-like substance is present in most eukaryotic
cells, primarily in the mitochondria. It is a component of the electron transport chain
and participates in aerobic cellular respiration, generating energy in the form of ATP
. Ninety-five percent of the human body’s energy is generated this way. Therefore, those organs with the highest energy requirements—such as the heart, liver and kidney —have the highest CoQ10 concentrations. There are three redox states of coenzyme Q10: fully oxidized (ubiquinone), semiquinone (ubisemiquinone), and fully reduced (ubiquinol
). The capacity of this molecule to exist in a completely oxidized form and a completely reduced form enables it to perform its functions in electron transport chain and as an antioxidant respectively.
Enzyme Institute in 1957. In 1958, its chemical structure was reported by Dr. Karl Folkers and coworkers at Merck; in 1968, Folkers became a Professor in the Chemistry Department at the University of Texas at Austin
. In 1961 Peter Mitchel proposed the electron transport chain (which includes the vital protonmotive role of CoQ10) and he received a Nobel prize for the same in 1978. In 1972, Gian Paolo Littarru and Karl Folkers separately demonstrated a deficiency of CoQ10 in human heart disease. The 1980s witnessed a steep rise in the number of clinical trials due to the availability of large quantities of pure CoQ10 and methods to measure plasma and blood CoQ10 concentrations. The antioxidant role of the molecule as a free radical scavenger was widely studied by Lars Ernster. Numerous scientists around the globe started studies on this molecule since then in relation to various diseases including cardiovascular diseases and cancer.
subunits in their side-chains. The most common Coenzyme Q in human mitochondria is CoQ10. Q refers to the quinone head and 10 refers to the number of isoprene repeats in the tail. The image below has three isoprenoid
units and would be called Q3.
 CoQ10 is found in the membranes
CoQ10 is found in the membranes
of many organelles. Since its primary function in cells is in generating energy, the highest concentration is found on the inner membrane
of the mitochondrion
. Some other organelles that contain CoQ10 include endoplasmic reticulum
, peroxisome
s, lysosome
s, and vesicle
s.
Genes involved include PDSS1
, PDSS2
, COQ2
, and COQ8/CABC1
.
, another lipid-soluble nutrient.This process in the human body involves the secretion of pancreatic enzymes and bile into the small intestines that facilitate emulsification and micelle formation that is required for the absorption of lipophilic substances. Food intake (and the presence of lipids) stimulates bodily biliary excretion of bile acids and greatly enhances the absorption of CoQ10. Exogenous CoQ10 is absorbed from the small intestinal tract and is best absorbed if it is taken with a meal. Serum concentration of CoQ10 in fed condition is higher than in fasting conditions.
CoQ10 in rat
s showed most of the radioactivity in the liver 2 hours after oral administration when the peak plasma radioactivity was observed, but it should be noted that CoQ9 is the predominant form of coenzyme Q in rats. It appears that CoQ10 is metabolised in all tissues, while a major route for its elimination is biliary and fecal excretion. After the withdrawal of CoQ10 supplementation, the levels return to normal within a few days, irrespective of the type of formulation used.
Toxicity is not usually observed with high doses of CoQ10. A daily dosage up to 3600 mg was found to be tolerated by healthy as well as unhealthy persons. However, some adverse effects, largely gastrointestinal, are reported with very high intakes. The observed safe level (OSL) risk assessment method indicated that the evidence of safety is strong at intakes up to 1200 mg/day, and this level is identified as the OSL.
Culture fibroblasts can be used also to evaluate the rate of endogenous CoQ10 biosynthesis, by measuring the uptake of 14C-labelled p-hydroxybenzoate.
. The synthesis of an intermediary precursor of coenzyme Q10, mevalonate, is inhibited by some beta blocker
s, blood pressure-lowering medication, and statins, a class of cholesterol-lowering drugs. Statins can reduce serum levels of coenzyme Q10 by up to 40%. Some research suggests the logical option of supplementation with coenzyme Q10 as a routine adjunct to any treatment that may reduce endogenous
production of coenzyme Q10, based on a balance of likely benefit against very small risk.. However, there are still no conclusive data that support the role of CoQ10 deficiency in the pathogenesis of statin-related myopathy.
polymer
, formulations based on various solubilising agents, i.e., hydrogenated lecithin
, and complexation with cyclodextrins; among the latter, complex with β-cyclodextrin has been found to have highly increased bioavailability. and is also used in pharmaceutical and food industry for CoQ10-fortification. Also some other novel carrier systems like liposomes, nanoparticles, dendrimers etc. can be used to increase the bioavailability of Coenzyme Q10.
in the United States
after Omega-3 and multivitamins.
According to the Mayo Clinic
, "CoQ10 has been used, recommended, or studied for numerous conditions, but remains controversial as a treatment in many areas." Coenzyme Q-10 is approved for use as an orphan product in the treatment of Huntington's disease
and mitochondrial cytopathies; other uses are still unproven, including in the treatment of congestive heart failure and athletic performance.
Oxidation of the circulating LDL is thought to play a key role in the pathogenesis of atherosclerosis, which is the underlying disorder leading to heart attack and ischemic strokes and CHD. Studies in the last decade have demonstrated that the content of Ubiquinol
in human LDL affords protection against the oxidative modifications of LDL themselves, thus lowering their atherogenic potency.
headaches. So far, three studies have been done, of which two were small, did not have a placebo group, were not randomized, and were open-label
, and one was a double-blind, randomized, placebo-controlled trial, which found statistically significant results despite its small sample size of 42 patients. Dosages were 150 to 300 mg/day.
It has been used effectively in the prophylaxis of migraines, especially in combination with a daily supplement of magnesium citrate
500 mg and riboflavin
(vitamin B2) 400 mg.
, and as relief from cancer treatment side-effects.
A recent (2007) meta-analysis of the clinical trials of CoQ10 for hypertension reviewed all published trials of coenzyme Q10 for hypertension
, and assessed overall efficacy, consistency of therapeutic action, and side-effect incidence. Meta-analysis was performed in 12 clinical trials (362 patients) comprising three randomized controlled trials, one crossover study, and eight open-label studies. The meta-analysis concluded that coenzyme Q10 has the potential in hypertensive patients to lower systolic blood pressure by up to 17 mm Hg and diastolic blood pressure by up to 10 mm Hg without significant side-effects.
conditions.
double-strand breaks, and a combination of a diet rich in polyunsaturated fatty acids and coenzyme Q10 supplementation leads to a longer lifespan in rats. Coles and Harris demonstrated an extension in the lifespan of rats when they were given coenzyme Q10 supplementation. But multiple studies have since found no increase in lifespan or decrease in aging in mice and rats supplemented with coenzyme Q10. Another study demonstrated that coenzyme Q10 extends the lifespan of C. elegans (nematode).
experiments, coenzyme Q10 taken as dietary supplement reduced radiation damage to the animals' blood.
patients found 1200 mg/day reduced the progression by 44%. and a phase III trial of 1200 mg/d and 2400 mg/d should run until 2011.
Meat and fish are the richest source of dietary CoQ10 and levels over 50 mg/kg can be found in beef, pork and chicken heart, and chicken liver. Dairy products are much poorer sources of CoQ10 compared to animal tissues. Vegetable oils are also quite rich in CoQ10. Within vegetables, parsley, and perilla are the richest CoQ10 sources, but significant differences in their CoQ10 levels can be found in the literature. Broccoli, grape, and cauliflower are modest sources of CoQ10. Most fruit and berries represent a poor to very poor source of CoQ10, with the exception of avocado, with a relatively high CoQ10 content.
1,4-Benzoquinone
1,4-Benzoquinone, commonly known as para-quinone, is a chemical compound with the formula C6H4O2. In a pure state, it forms bright-yellow crystals with a characteristic irritating odor, resembling that of chlorine, bleach, and hot plastic. Impure samples are often dark-colored due to the presence...
, where Q refers to the quinone
Quinone
A quinone is a class of organic compounds that are formally "derived from aromatic compounds [such as benzene or naphthalene] by conversion of an even number of –CH= groups into –C– groups with any necessary rearrangement of double bonds," resulting in "a fully conjugated cyclic dione structure."...
chemical group, and 10 refers to the number of isoprenyl
Isoprene
Isoprene , or 2-methyl-1,3-butadiene, is a common organic compound with the formula CH2=CCH=CH2. Under standard conditions it is a colorless liquid...
chemical subunits in its tail.
This oil-soluble, vitamin-like substance is present in most eukaryotic
Eukaryote
A eukaryote is an organism whose cells contain complex structures enclosed within membranes. Eukaryotes may more formally be referred to as the taxon Eukarya or Eukaryota. The defining membrane-bound structure that sets eukaryotic cells apart from prokaryotic cells is the nucleus, or nuclear...
cells, primarily in the mitochondria. It is a component of the electron transport chain
Electron transport chain
An electron transport chain couples electron transfer between an electron donor and an electron acceptor with the transfer of H+ ions across a membrane. The resulting electrochemical proton gradient is used to generate chemical energy in the form of adenosine triphosphate...
and participates in aerobic cellular respiration, generating energy in the form of ATP
Adenosine triphosphate
Adenosine-5'-triphosphate is a multifunctional nucleoside triphosphate used in cells as a coenzyme. It is often called the "molecular unit of currency" of intracellular energy transfer. ATP transports chemical energy within cells for metabolism...
. Ninety-five percent of the human body’s energy is generated this way. Therefore, those organs with the highest energy requirements—such as the heart, liver and kidney —have the highest CoQ10 concentrations. There are three redox states of coenzyme Q10: fully oxidized (ubiquinone), semiquinone (ubisemiquinone), and fully reduced (ubiquinol
Ubiquinol
Ubiquinol is an electron-rich form of coenzyme Q10.The natural ubiquinol form of coenzyme Q10 is 2,3-dimethoxy-5-methyl-6-poly prenyl-1,4-benzoquinol, where the polyprenylated side chain is 9-10 units long in mammals...
). The capacity of this molecule to exist in a completely oxidized form and a completely reduced form enables it to perform its functions in electron transport chain and as an antioxidant respectively.
Discovery and history
Coenzyme Q10 was first discovered by Professor Fredrick L. Crane and colleagues at the University of Wisconsin–MadisonUniversity of Wisconsin–Madison
The University of Wisconsin–Madison is a public research university located in Madison, Wisconsin, United States. Founded in 1848, UW–Madison is the flagship campus of the University of Wisconsin System. It became a land-grant institution in 1866...
Enzyme Institute in 1957. In 1958, its chemical structure was reported by Dr. Karl Folkers and coworkers at Merck; in 1968, Folkers became a Professor in the Chemistry Department at the University of Texas at Austin
University of Texas at Austin
The University of Texas at Austin is a state research university located in Austin, Texas, USA, and is the flagship institution of the The University of Texas System. Founded in 1883, its campus is located approximately from the Texas State Capitol in Austin...
. In 1961 Peter Mitchel proposed the electron transport chain (which includes the vital protonmotive role of CoQ10) and he received a Nobel prize for the same in 1978. In 1972, Gian Paolo Littarru and Karl Folkers separately demonstrated a deficiency of CoQ10 in human heart disease. The 1980s witnessed a steep rise in the number of clinical trials due to the availability of large quantities of pure CoQ10 and methods to measure plasma and blood CoQ10 concentrations. The antioxidant role of the molecule as a free radical scavenger was widely studied by Lars Ernster. Numerous scientists around the globe started studies on this molecule since then in relation to various diseases including cardiovascular diseases and cancer.
Chemical properties
The oxidized structure of CoQ10 is shown on the top-right. The various kinds of Coenzyme Q can be distinguished by the number of isoprenoidIsoprene
Isoprene , or 2-methyl-1,3-butadiene, is a common organic compound with the formula CH2=CCH=CH2. Under standard conditions it is a colorless liquid...
subunits in their side-chains. The most common Coenzyme Q in human mitochondria is CoQ10. Q refers to the quinone head and 10 refers to the number of isoprene repeats in the tail. The image below has three isoprenoid
Isoprene
Isoprene , or 2-methyl-1,3-butadiene, is a common organic compound with the formula CH2=CCH=CH2. Under standard conditions it is a colorless liquid...
units and would be called Q3.
Biochemical role
Biological membrane
A biological membrane or biomembrane is an enclosing or separatingmembrane that acts as a selective barrier, within or around a cell. It consists of a lipid bilayer with embedded proteins that may constitute close to 50% of membrane content...
of many organelles. Since its primary function in cells is in generating energy, the highest concentration is found on the inner membrane
Biological membrane
A biological membrane or biomembrane is an enclosing or separatingmembrane that acts as a selective barrier, within or around a cell. It consists of a lipid bilayer with embedded proteins that may constitute close to 50% of membrane content...
of the mitochondrion
Mitochondrion
In cell biology, a mitochondrion is a membrane-enclosed organelle found in most eukaryotic cells. These organelles range from 0.5 to 1.0 micrometers in diameter...
. Some other organelles that contain CoQ10 include endoplasmic reticulum
Endoplasmic reticulum
The endoplasmic reticulum is an organelle of cells in eukaryotic organisms that forms an interconnected network of tubules, vesicles, and cisternae...
, peroxisome
Peroxisome
Peroxisomes are organelles found in virtually all eukaryotic cells. They are involved in the catabolism of very long chain fatty acids, branched chain fatty acids, D-amino acids, polyamines, and biosynthesis of plasmalogens, etherphospholipids critical for the normal function of mammalian brains...
s, lysosome
Lysosome
thumb|350px|Schematic of typical animal cell, showing subcellular components. [[Organelle]]s: [[nucleoli]] [[cell nucleus|nucleus]] [[ribosomes]] [[vesicle |vesicle]] rough [[endoplasmic reticulum]]...
s, and vesicle
Vesicle (biology)
A vesicle is a bubble of liquid within another liquid, a supramolecular assembly made up of many different molecules. More technically, a vesicle is a small membrane-enclosed sack that can store or transport substances. Vesicles can form naturally because of the properties of lipid membranes , or...
s.
CoQ10 and electron transport chain
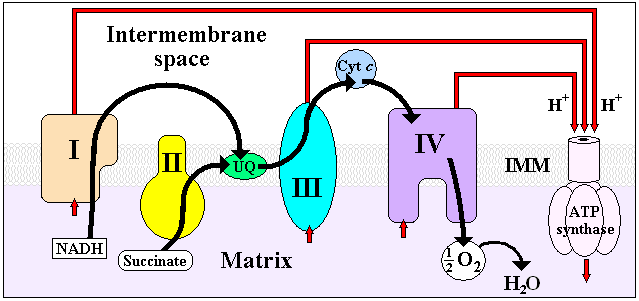
CoQ10 is fat-soluble and is therefore mobile in cellular membranes; it plays a unique role in the electron transport chain (ETC). In the inner mitochondrial membrane, electrons from NADH and succinate pass through the ETC to the oxygen, which is then reduced to water. The transfer of electrons through ETC results in the pumping of H+ across the membrane creating a proton gradient across the membrane, which is used by ATP synthase (located on the membrane) to generate ATP. CoQ10 functions as an electron carrier from enzyme complex I and enzyme complex II to complex III in this process. This is crucial in the process, since no other molecule can perform this function. Thus, CoQ10 functions in every cell of the body to synthesize energy.Antioxidant function of CoQ10
The antioxidant nature of CoQ10 derives from its energy carrier function. As an energy carrier, the CoQ10 molecule is continually going through an oxidation-reduction cycle. As it accepts electrons, it becomes reduced. As it gives up electrons, it becomes oxidized. In its reduced form, the CoQ10 molecule holds electrons rather loosely, so this CoQ molecule will quite easily give up one or both electrons and, thus, act as an antioxidant. CoQ10 inhibits lipid peroxidation by preventing the production of lipid peroxyl radicals (LOO). Moreover, CoQH2 reduces the initial perferryl radical and singlet oxygen, with concomitant formation of ubisemiquinone and H2O2. This quenching of the initiating perferryl radicals, which prevent propagation of lipid peroxidation, protects not only lipids, but also proteins from oxidation. In addition, the reduced form of CoQ effectively regenerates vitamin E from the a-tocopheroxyl radical, thereby interfering with the propagation step. Furthermore, during oxidative stress, interaction of H2O2 with metal ions bound to DNA generates hydroxyl radicals and CoQ efficiently prevents the oxidation of bases, in particular, in mitochondrial DNA. In contrast to other antioxidants, this compound inhibits both the initiation and the propagation of lipid and protein oxidation. It also regenerates other antioxidants such as vitamin E. The circulating CoQ10 in LDL prevents oxidation of LDL, therefore, by providing its benefits in cardiovascular diseases.Biosynthesis
Starting from acetyl-CoA, a multistep process of mevalonate pathway produces farnesyl-PP (FPP), the precursor for cholesterol, CoQ, dolichol, and isoprenylated proteins. An important enzyme in this pathway is HMG Co-A reductase, which is usually a target for intervention in cardiovascular complications. The long isoprenoid side-chain of CoQ is synthesized by trans-prenyltransferase, which condenses FPP with several molecules of isopentenyl-PP (IPP), all in the trans configuration. The next step involves condensation of this polyisoprenoid side-chain with 4-hydroxybenzoate, catalyzed by polyprenyl-4-hydroxy benzoate transferase. Hydroxybenzoate is synthesized from tyrosine or phenylalanine. In addition to their presence in mitochondria, these initial two reactions also occur in the endoplasmic reticulum and peroxisomes, indicating multiple sites of synthesis in animal cells. Increasing the endogenous biosynthesis of CoQ10 has attained attention in the recent years as a strategy to fight CoQ10 deficiency.Genes involved include PDSS1
PDSS1
Decaprenyl-diphosphate synthase subunit 1 is an enzyme that in humans is encoded by the PDSS1 gene.-Further reading:...
, PDSS2
PDSS2
Decaprenyl-diphosphate synthase subunit 2 , also known as candidate tumor suppressor protein, is a protein that in humans is encoded by the PDSS2 gene.- Function :...
, COQ2
COQ2
Para-hydroxybenzoate--polyprenyltransferase, mitochondrial is an enzyme that in humans is encoded by the COQ2 gene.-Further reading:...
, and COQ8/CABC1
CABC1
Chaperone activity of bc1 complex-like, mitochondrial is a protein that in humans is encoded by the CABC1 gene.-Further reading:...
.
Absorption
CoQ10 is a crystalline powder that is insoluble in water. Absorption follows the same process as that of lipids and the uptake mechanism appears to be similar to that of vitamin EVitamin E
Vitamin E is used to refer to a group of fat-soluble compounds that include both tocopherols and tocotrienols. There are many different forms of vitamin E, of which γ-tocopherol is the most common in the North American diet. γ-Tocopherol can be found in corn oil, soybean oil, margarine and dressings...
, another lipid-soluble nutrient.This process in the human body involves the secretion of pancreatic enzymes and bile into the small intestines that facilitate emulsification and micelle formation that is required for the absorption of lipophilic substances. Food intake (and the presence of lipids) stimulates bodily biliary excretion of bile acids and greatly enhances the absorption of CoQ10. Exogenous CoQ10 is absorbed from the small intestinal tract and is best absorbed if it is taken with a meal. Serum concentration of CoQ10 in fed condition is higher than in fasting conditions.
Metabolism
Data on the metabolism of CoQ10 in animals and humans are limited. A study with 14C-labeledCarbon-14
Carbon-14, 14C, or radiocarbon, is a radioactive isotope of carbon with a nucleus containing 6 protons and 8 neutrons. Its presence in organic materials is the basis of the radiocarbon dating method pioneered by Willard Libby and colleagues , to date archaeological, geological, and hydrogeological...
CoQ10 in rat
Rat
Rats are various medium-sized, long-tailed rodents of the superfamily Muroidea. "True rats" are members of the genus Rattus, the most important of which to humans are the black rat, Rattus rattus, and the brown rat, Rattus norvegicus...
s showed most of the radioactivity in the liver 2 hours after oral administration when the peak plasma radioactivity was observed, but it should be noted that CoQ9 is the predominant form of coenzyme Q in rats. It appears that CoQ10 is metabolised in all tissues, while a major route for its elimination is biliary and fecal excretion. After the withdrawal of CoQ10 supplementation, the levels return to normal within a few days, irrespective of the type of formulation used.
CoQ10 deficiency and toxicity
There are two major factors that lead to deficiency of CoQ10 in humans: reduced biosynthesis, and increased utilization by the body. Biosynthesis is the major source of CoQ10. Biosynthesis requires at least 12 genes, and mutations in many of them cause CoQ deficiency. CoQ10 levels can also can be affected by other genetic defects (such as mutations of mitochondrial DNA, ETFDH, APTX and BRAF, genes that are not directly related to the CoQ10 biosynthetic process) while the role of statins is controversial. Some chronic disease conditions (cancer, heart disease, etc.) are also thought to reduce the biosynthesis and increase the demand for CoQ10 in the body, but there is no definite data to support these claims.Toxicity is not usually observed with high doses of CoQ10. A daily dosage up to 3600 mg was found to be tolerated by healthy as well as unhealthy persons. However, some adverse effects, largely gastrointestinal, are reported with very high intakes. The observed safe level (OSL) risk assessment method indicated that the evidence of safety is strong at intakes up to 1200 mg/day, and this level is identified as the OSL.
Clinical assessment techniques
Although CoQ10 can be measured in plasma, these measurements reflect dietary intake rather than tissue status. Currently, most clinical centers measure CoQ10 levels in cultured skin fibroblasts, muscle biopsies, and in blood mononuclear cells.Culture fibroblasts can be used also to evaluate the rate of endogenous CoQ10 biosynthesis, by measuring the uptake of 14C-labelled p-hydroxybenzoate.
Inhibition by statins and beta blockers
Coenzyme Q10 shares a biosynthetic pathway with cholesterolCholesterol
Cholesterol is a complex isoprenoid. Specifically, it is a waxy steroid of fat that is produced in the liver or intestines. It is used to produce hormones and cell membranes and is transported in the blood plasma of all mammals. It is an essential structural component of mammalian cell membranes...
. The synthesis of an intermediary precursor of coenzyme Q10, mevalonate, is inhibited by some beta blocker
Beta blocker
Beta blockers or beta-adrenergic blocking agents, beta-adrenergic antagonists, beta-adrenoreceptor antagonists or beta antagonists, are a class of drugs used for various indications. They are particularly for the management of cardiac arrhythmias, cardioprotection after myocardial infarction ,...
s, blood pressure-lowering medication, and statins, a class of cholesterol-lowering drugs. Statins can reduce serum levels of coenzyme Q10 by up to 40%. Some research suggests the logical option of supplementation with coenzyme Q10 as a routine adjunct to any treatment that may reduce endogenous
Endogenous
Endogenous substances are those that originate from within an organism, tissue, or cell. Endogenous retroviruses are caused by ancient infections of germ cells in humans, mammals and other vertebrates...
production of coenzyme Q10, based on a balance of likely benefit against very small risk.. However, there are still no conclusive data that support the role of CoQ10 deficiency in the pathogenesis of statin-related myopathy.
Pharmacokinetics
Some reports have been published on the pharmacokinetics of CoQ10. The plasma peak can be observed 2–6 hours after oral administration, mainly depending on the design of the study. In some studies, a second plasma peak was also observed at about 24 hours after administration, probably due to both enterohepatic recycling and redistribution from the liver to circulation. Tomono et al. used deuterium-labelled crystalline CoQ10 to investigate pharmacokinetics in human and determined an elimination half-time of 33 hours.Improving the bioavailability of CoQ10
The importance of how drugs are formulated for bioavailability is well known. In order to find a principle to boost the bioavailability of CoQ10 after oral administration, several new approaches have been taken and different formulations, and forms have been developed and tested on animals or humans.Reduction of particle size
An obvious strategy is reduction of the particle size to as low as the micro- and nano-scale. Nanoparticles have been explored as a delivery system for various drugs and an improvement of the oral bioavailability of drugs with poor absorption characteristics has been reported; the pathways of absorption and the efficiency were affected by reduction of particle size. This protocol has so far not proved to be very successful with CoQ10, although reports have differed widely. The use of the aqueous suspension of finely powdered CoQ10 in pure water has also revealed only a minor effect.Soft-gel capsules with CoQ10 in oil suspension
A successful approach was to use the emulsion system to facilitate absorption from the gastrointestinal tract and to improve bioavailability. Emulsions of soybean oil (lipid microspheres) could be stabilised very effectively by lecithin and were utilised in the preparation of soft gelatine capsules. In one of the first such attempts, Ozawa et al. performed a pharmacokinetic study on beagle dogs in which the emulsion of CoQ10 in soybean oil was investigated; about two times higher plasma CoQ10 level than that of the control tablet preparation was determined during administration of a lipid microsphere. Although an almost negligible improvement of bioavailability was observed by Kommuru et al. with oil-based soft-gel capsules in a later study on dogs, the significantly increased bioavailability of CoQ10 was confirmed for several oil-based formulations in most other studies.Novel forms of CoQ10 with increased water-solubility
Facilitating drug absorption by increasing its solubility in water is a common pharmaceutical strategy and has also been shown to be successful for Coenzyme Q10. Various approaches have been developed to achieve this goal, with many of them producing significantly better results over oil-based soft-gel capsules in spite of the many attempts to optimize their composition. Examples of such approaches are use of the aqueous dispersion of solid CoQ10 with tyloxapolTyloxapol
Tyloxapol is a nonionic liquid polymer of the alkyl aryl polyether alcohol type. It is used as a surfactant to aid liquefaction and removal of mucopurulent bronchopulmonary secretions, administered by inhalation through a nebulizer or with a stream of oxygen.With intraperitoneal injection,...
polymer
Polymer
A polymer is a large molecule composed of repeating structural units. These subunits are typically connected by covalent chemical bonds...
, formulations based on various solubilising agents, i.e., hydrogenated lecithin
Lecithin
Lecithin is a generic term to designate any group of yellow-brownish fatty substances occurring in animal and plant tissues, and in egg yolk, composed of phosphoric acid, choline, fatty acids, glycerol, glycolipids, triglycerides, and phospholipids .The word lecithin was originally coined in 1847 by...
, and complexation with cyclodextrins; among the latter, complex with β-cyclodextrin has been found to have highly increased bioavailability. and is also used in pharmaceutical and food industry for CoQ10-fortification. Also some other novel carrier systems like liposomes, nanoparticles, dendrimers etc. can be used to increase the bioavailability of Coenzyme Q10.
Supplementation benefits
Coenzyme Q10 is the 3rd most sold dietary ingredientDietary supplement
A dietary supplement, also known as food supplement or nutritional supplement, is a preparation intended to supplement the diet and provide nutrients, such as vitamins, minerals, fiber, fatty acids, or amino acids, that may be missing or may not be consumed in sufficient quantities in a person's diet...
in the United States
United States
The United States of America is a federal constitutional republic comprising fifty states and a federal district...
after Omega-3 and multivitamins.
According to the Mayo Clinic
Mayo Clinic
Mayo Clinic is a not-for-profit medical practice and medical research group specializing in treating difficult patients . Patients are referred to Mayo Clinic from across the U.S. and the world, and it is known for innovative and effective treatments. Mayo Clinic is known for being at the top of...
, "CoQ10 has been used, recommended, or studied for numerous conditions, but remains controversial as a treatment in many areas." Coenzyme Q-10 is approved for use as an orphan product in the treatment of Huntington's disease
Huntington's disease
Huntington's disease, chorea, or disorder , is a neurodegenerative genetic disorder that affects muscle coordination and leads to cognitive decline and dementia. It typically becomes noticeable in middle age. HD is the most common genetic cause of abnormal involuntary writhing movements called chorea...
and mitochondrial cytopathies; other uses are still unproven, including in the treatment of congestive heart failure and athletic performance.
Heart health
Coenzyme Q10 helps to maintain a healthy cardiovascular system. There is evidence of CoQ10 deficiency in heart failure. Recently, CoQ10 plasma concentrations have been demonstrated as an independent predictor of mortality in chronic heart failure, CoQ10 deficiency being detrimental to the long-term prognosis of chronic heart failure. CoQ10 is available as medicine in several European countries, but is in these countries also available as a food supplement.Oxidation of the circulating LDL is thought to play a key role in the pathogenesis of atherosclerosis, which is the underlying disorder leading to heart attack and ischemic strokes and CHD. Studies in the last decade have demonstrated that the content of Ubiquinol
Ubiquinol
Ubiquinol is an electron-rich form of coenzyme Q10.The natural ubiquinol form of coenzyme Q10 is 2,3-dimethoxy-5-methyl-6-poly prenyl-1,4-benzoquinol, where the polyprenylated side chain is 9-10 units long in mammals...
in human LDL affords protection against the oxidative modifications of LDL themselves, thus lowering their atherogenic potency.
Migraine headaches
Supplementation of coenzyme Q10 has been found to have a beneficial effect on the condition of some sufferers of migraineMigraine
Migraine is a chronic neurological disorder characterized by moderate to severe headaches, and nausea...
headaches. So far, three studies have been done, of which two were small, did not have a placebo group, were not randomized, and were open-label
Open-label trial
An open-label trial or open trial is a type of clinical trial in which both the researchers and participants know which treatment is being administered....
, and one was a double-blind, randomized, placebo-controlled trial, which found statistically significant results despite its small sample size of 42 patients. Dosages were 150 to 300 mg/day.
It has been used effectively in the prophylaxis of migraines, especially in combination with a daily supplement of magnesium citrate
Magnesium citrate
Magnesium citrate, a magnesium salt of citric acid, is a chemical agent used medicinally as a saline laxative and to completely empty the bowel prior to a major surgery or colonoscopy. It is available without a prescription, both as a generic brand or under the brand name Citromag or Citroma. It is...
500 mg and riboflavin
Riboflavin
Riboflavin, also known as vitamin B2 or additive E101, is an easily absorbed micronutrient with a key role in maintaining health in humans and animals. It is the central component of the cofactors FAD and FMN, and is therefore required by all flavoproteins. As such, vitamin B2 is required for a...
(vitamin B2) 400 mg.
Cancer
CoQ10 is also being investigated as a treatment for cancerCancer
Cancer , known medically as a malignant neoplasm, is a large group of different diseases, all involving unregulated cell growth. In cancer, cells divide and grow uncontrollably, forming malignant tumors, and invade nearby parts of the body. The cancer may also spread to more distant parts of the...
, and as relief from cancer treatment side-effects.
Cardiac arrest
Another recent study shows a survival benefit after cardiac arrest if coenzyme Q10 is administered in addition to commencing active cooling of the body to 90–93 degrees Fahrenheit (32–34 degrees Celsius).Blood pressure
There are several reports concerning the effect of CoQ10 on blood pressure in human studies.A recent (2007) meta-analysis of the clinical trials of CoQ10 for hypertension reviewed all published trials of coenzyme Q10 for hypertension
Hypertension
Hypertension or high blood pressure is a cardiac chronic medical condition in which the systemic arterial blood pressure is elevated. What that means is that the heart is having to work harder than it should to pump the blood around the body. Blood pressure involves two measurements, systolic and...
, and assessed overall efficacy, consistency of therapeutic action, and side-effect incidence. Meta-analysis was performed in 12 clinical trials (362 patients) comprising three randomized controlled trials, one crossover study, and eight open-label studies. The meta-analysis concluded that coenzyme Q10 has the potential in hypertensive patients to lower systolic blood pressure by up to 17 mm Hg and diastolic blood pressure by up to 10 mm Hg without significant side-effects.
Periodontal disease
Studies have shown that diseased gum tissue is deficient in CoQ10 compared to healthy gum tissue. Human clinical trials have suggested a link between oral administration of CoQ10 and improved gingival health, immune response in gum tissues, and a reversal of the diseased gum conditions. In addition to oral supplementation, topical application of CoQ10 on gum tissues has been shown to improve periodontitis and gingivitisGingivitis
Gingivitis is a term used to describe non-destructive periodontal disease. The most common form of gingivitis is in response to bacterial biofilms adherent to tooth surfaces, termed plaque-induced gingivitis, and is the most common form of periodontal disease...
conditions.
Lifespan
One study demonstrated that low dosages of coenzyme Q10 reduce oxidation and DNADNA
Deoxyribonucleic acid is a nucleic acid that contains the genetic instructions used in the development and functioning of all known living organisms . The DNA segments that carry this genetic information are called genes, but other DNA sequences have structural purposes, or are involved in...
double-strand breaks, and a combination of a diet rich in polyunsaturated fatty acids and coenzyme Q10 supplementation leads to a longer lifespan in rats. Coles and Harris demonstrated an extension in the lifespan of rats when they were given coenzyme Q10 supplementation. But multiple studies have since found no increase in lifespan or decrease in aging in mice and rats supplemented with coenzyme Q10. Another study demonstrated that coenzyme Q10 extends the lifespan of C. elegans (nematode).
Radiation injury
A 2002 study reported that, in ratLaboratory rat
A laboratory rat is a rat of the species Rattus norvegicus which is bred and kept for scientific research. Laboratory rats have served as an important animal model for research in psychology, medicine, and other fields.- Origins :...
experiments, coenzyme Q10 taken as dietary supplement reduced radiation damage to the animals' blood.
Parkinson's disease
A 2002 study in 80 Parkinson's diseaseParkinson's disease
Parkinson's disease is a degenerative disorder of the central nervous system...
patients found 1200 mg/day reduced the progression by 44%. and a phase III trial of 1200 mg/d and 2400 mg/d should run until 2011.
Coenzyme Q10 concentrations in foods and dietary intake
Detailed reviews on occurrence of CoQ10 and dietary intake were published recently. Besides endogenous synthesis, CoQ10 is also supplied to the organism by various foods. However, despite the scientific community’s great interest in this compound, a very limited number of studies have been performed to determine the contents of CoQ10 in dietary components. The first reports on this issue were published in 1959, but the sensitivity and selectivity of the analytical methods at that time did not allow reliable analyses, especially for products with low concentrations. Developments in analytical chemistry have since enabled a more reliable determination of CoQ10 concentrations in various foods (Table below).| Food | Coenzyme Q10 concentration [mg/kg] |
|---|---|
| Beef | |
| heart | 113 |
| liver | 39–50 |
| muscle | 26–40 |
| Pork | |
| heart | 11.8–128.2 |
| liver | 22.7–54.0 |
| muscle | 13.8–45.0 |
| Chicken | |
| heart | 116.2–132.2 |
| Fish | |
| sardine | 5–64 |
| mackerel | |
| red flesh | 43–67 |
| white flesh | 11–16 |
| salmon | 4–8 |
| tuna | 5 |
| Oils | |
| soybean | 54–280 |
| olive | 4–160 |
| grapeseed | 64–73 |
| sunflower | 4–15 |
| rice bran | / |
| coconut | |
| Nuts | |
| peanuts | 27 |
| walnuts | 19 |
| sesame seeds | 18–23 |
| pistachio nuts | 20 |
| hazelnuts | 17 |
| almond | 5–14 |
| Vegetables | |
| parsley | 8–26 |
| broccoli | 6–9 |
| cauliflower | 2–7 |
| spinach | up to 10 |
| grape | 6–7 |
| Chinese cabbage | 2–5 |
| Fruit | |
| avocado | 10 |
| blackcurrant | 3 |
| strawberry | 1 |
| orange | 1–2 |
| grapefruit | 1 |
| apple | 1 |
Meat and fish are the richest source of dietary CoQ10 and levels over 50 mg/kg can be found in beef, pork and chicken heart, and chicken liver. Dairy products are much poorer sources of CoQ10 compared to animal tissues. Vegetable oils are also quite rich in CoQ10. Within vegetables, parsley, and perilla are the richest CoQ10 sources, but significant differences in their CoQ10 levels can be found in the literature. Broccoli, grape, and cauliflower are modest sources of CoQ10. Most fruit and berries represent a poor to very poor source of CoQ10, with the exception of avocado, with a relatively high CoQ10 content.
Intake
In the developed world, the estimated daily intake of CoQ10 has been determined at 3–6 mg per day, derived primarily from meat.See also
- IdebenoneIdebenoneIdebenone is an experimental drug, initially developed by Takeda Pharmaceutical Company for the treatment of Alzheimer's disease and other cognitive defects. This has been met with limited success. The Swiss company Santhera Pharmaceuticals has started to investigate it for the treatment of...
– synthetic analog with reduced oxidant generating properties - UbiquinolUbiquinolUbiquinol is an electron-rich form of coenzyme Q10.The natural ubiquinol form of coenzyme Q10 is 2,3-dimethoxy-5-methyl-6-poly prenyl-1,4-benzoquinol, where the polyprenylated side chain is 9-10 units long in mammals...
External links
- Coenzyme Q10: An Antioxidant Drug – from the Huntington's Disease Outreach Project for Education at StanfordHuntington's Disease Outreach Project for Education at StanfordThe Huntington’s disease Outreach Project for Education at Stanford is a student-run project at Stanford University dedicated to making scientific information about Huntington’s disease more readily accessible to patients and the public. Initiated by Professor William H...
- List of USP Verified CoQ10 Ingredients
- Detailed discussion of coenzyme q10 health benefits
- National Cancer Institute page on Coenzyme Q10
- Robert Alan Bonakdar and Erminia Guarneri, American Family Physician page on Coenzyme Q10
- An Introduction to Coenzyme Q10 at University of WashingtonUniversity of WashingtonUniversity of Washington is a public research university, founded in 1861 in Seattle, Washington, United States. The UW is the largest university in the Northwest and the oldest public university on the West Coast. The university has three campuses, with its largest campus in the University...
- Possible Health Benefits of Coenzyme Q10 at Oregon State UniversityOregon State UniversityOregon State University is a coeducational, public research university located in Corvallis, Oregon, United States. The university offers undergraduate, graduate and doctoral degrees and a multitude of research opportunities. There are more than 200 academic degree programs offered through the...
- Study Suggests Coenzyme Q10 Slows Functional Decline in Parkinson's Disease at National Institute of Neurological Disorders and StrokeNational Institute of Neurological Disorders and StrokeThe National Institute of Neurological Disorders and Stroke is a part of the U.S. National Institutes of Health . It conducts and funds research on brain and nervous system disorders and has a budget of just over US$1.5 billion...